John Reidy, Nigel Hacking and Bruce McLucas (eds.)Medical RadiologyRadiological Interventions in Obstetrics and Gynaecology201410.1007/174_2014_962
© Springer-Verlag Berlin Heidelberg 2014
Who Can and Should do Uterine Artery Embolisation
(1)
Department of Radiology, Guy’s Hospital, London, SE1 9RT, UK
1 Introduction
The first report of uterine artery embolisation (UAE) as a primary treatment for uterine fibroids was in 1996 (Ravina et al. 1995). The leading author in this seminal paper was a gynaecologist and the radiological input was by neuroradiologists. Radiologists, particularly interventional radiologists (IRs) who had been embolising in great variety of clinical situations since the 1980s, seized on this new application with enthusiasm—here was an elective procedure for a common condition that was minimally invasive compared with the standard treatment which for most women was a major surgery and a hysterectomy.
Gynaecologists were generally less enthusiastic in their uptake and acceptance of this new procedure, but as the experience of UAE has increased and national medical societies and bodies representing both radiologists and gynaecologists gave it their cautious approval, it has become more generally accepted.
Most commonly, IR procedures are undertaken at the request of a specialist referring clinician but in some situations this may not be necessary. The guidelines for UAE have all recognised that women should be referred by a gynaecologist who has made a full clinical evaluation and has discussed the other and alternative treatments for fibroid disease. If it has been accepted that gynaecologists are essential in the workup for UAE, similarly IRs have assumed they are the only operators capable of offering an UAE service. Although these divisions of clinical practice and responsibility generally apply, they have been questioned.
There are a number of aspects of UAE that will be addressed here that should be addressed in the establishment of UAE service.
Each will be separately considered:
1
Is it necessary for all women to be seen and assessed by a specialised gynaecologist prior to UAE?
2
Should clinicians other than IRs carry out uterine artery embolisation?
3
If other clinicians, e.g. gynaecologists and cardiologists are to do UAE, what credentialing is necessary? Of course the same checks should apply to IRs.
4
Who should look after women immediately after UAE and be responsible for their in-hospital treatment?
5
In the event of early concerns or complications (<1 month), who should be responsible for their care?
6
Who should see women for their routine follow-up?
2 Is it Necessary for All Women to be Seen and Assessed by a Specialist Gynaecologist?
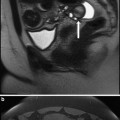
When a woman is referred to a gynaecologist by her family doctor, he will assess the clinical symptoms and signs, and will commonly make a clinical diagnosis of uterine fibroids backed up by some imaging, most commonly initial ultrasound. Many will now routinely request an MRI scan with contrast and there is a tendency for more MRIs to be requested even when there are cost considerations in the local clinical practice. When symptoms are considered to be significant and related to fibroids, the possible treatments of hysterectomy, myomectomy and UAE should be considered and discussed. If women are then referred for UAE, this can mean two hospital specialists are involved which may have financial implications.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


