Capillary hemangioma – postoperative radiosurgery for residual tumor
SKULL BASE REGION
Jugular foramen
HISTOPATHOLOGY
Capillary hemangioma
PRIOR SURGICAL RESECTION
Yes
PERTINENT LABORATORY FINDINGS
None
Case description
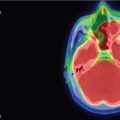
The patient is a 60-year-old male who presented with right unilateral conductive hearing loss associated with a reddish mass involving the inferior aspect of the tympanic membrane and the medial external auditory canal. He had no lower cranial nerve deficits prior to presentation. Magnetic resonance imaging (MRI) with contrast revealed an avidly enhancing lesion involving the middle ear with extension inferiorly to the lateral jugular bulb (ipsilateral dominant sinus) ( Figure 10.46.1 ). The location was a bit unusual for either a tympanic or jugular paraganglioma given that it was neither centered on the promontory nor the jugular bulb. In addition, it did not demonstrate the typical pattern of osseous erosion or prominent flow voids. The patient elected to undergo initial surgical resection for pathologic diagnosis, improvement of conductive hearing loss, and possible curative treatment. Intraoperatively, a subtotal resection was performed as the tumor involved the jugular bulb, and the surgeon elected to leave the dominant sinus intact. The lateral aspect of the tumor was removed and the patient’s conductive hearing loss resolved ( Figure 10.46.2 ). Although intraoperative frozen section pathology was consistent with paraganglioma, final pathology confirmed a diagnosis of intraosseous capillary hemangioma. Following subtotal resection, the patient and skull base team elected to treat the residual tumor with stereotactic radiosurgery (SRS) 6 months after surgery ( Figure 10.46.3 ).
Radiosurgery Machine
Gamma Knife
Radiosurgery Dose (Gy)
16 at the 50% isodose line
Number of Fractions
1
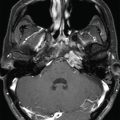
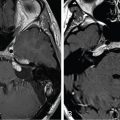
Figure 10.46.1.
A. Initial preoperative MRI: Axial T1-weighted image with gadolinium, showing a brightly enhancing lesion posterior and lateral to the vertical petrous carotid and possibly involving the lateral aspect of the jugular bulb. B. Initial preoperative CT: Axial cut showing a tumor within the external auditory canal. Of note, the jugular-carotid spine remained intact.
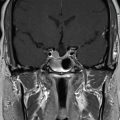
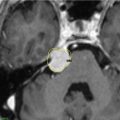
Figure 10.46.2.
Postoperative MRI, prior to stereotactic radiosurgery: Axial T1-weighted image with gadolinium showing a residual tumor surrounding the carotid and jugular foramen.
Only gold members can continue reading. Log In or Register to continue



 Esthesioneuroblastoma – delayed postoperative radiosurgery for recurrence at long-term
Esthesioneuroblastoma – delayed postoperative radiosurgery for recurrence at long-term
 Null cell – delayed postoperative radiosurgery for growing perioptic residual
Null cell – delayed postoperative radiosurgery for growing perioptic residual
 Suprasellar non-small cell lung carcinoma metastasis – upfront radiosurgery
Suprasellar non-small cell lung carcinoma metastasis – upfront radiosurgery
 Chondrosarcoma – definitive radiosurgery after subtotal resections
Chondrosarcoma – definitive radiosurgery after subtotal resections
 Large vestibular schwannoma – delayed postoperative radiosurgery for growing residual
Large vestibular schwannoma – delayed postoperative radiosurgery for growing residual
 Trigeminal neuralgia due to petroclival meningioma – upfront radiosurgery
Trigeminal neuralgia due to petroclival meningioma – upfront radiosurgery



