Cardiac Disease
Heart diseases frequently cause pulmonary dysfunction because of the close structural and functional association of the heart and lungs. The pulmonary vasculature is normally a low-pressure, low-resistance system with high compliance and a large vascular reserve. However, in patients with a left-to-right shunt due to congenital heart disease, the elevations in pulmonary artery flow and pressure result in progressive pathologic changes in the pulmonary vasculature. This leads to an increase in pulmonary vascular resistance, irreversible pulmonary hypertension, right-sided heart failure, and reversal of shunt flow, a condition known as Eisenmenger syndrome. In this chapter, the effects of cardiac disease on the pulmonary vasculature are examined. Atrial septal defect, ventricular septal defect, and patent ductus arteriosus are used as examples of congenital heart diseases with a left-to-right shunt. The lung changes, as seen on imaging, of acute and chronic pulmonary venous hypertension are explained, and the pulmonary vascular changes seen in the acquired heart disease mitral stenosis are illustrated.
 Atrial Septal Defect
Atrial Septal Defect
 Atrial septal defect accounts for one-third of cases of congenital heart disease detected in adults.
Atrial septal defect accounts for one-third of cases of congenital heart disease detected in adults.
 Ostium secundum atrial septal defects, the most common type, are located within the oval fossa; ostium primum atrial septal defects are next in frequency, and sinus venosus defects are the least common.
Ostium secundum atrial septal defects, the most common type, are located within the oval fossa; ostium primum atrial septal defects are next in frequency, and sinus venosus defects are the least common.
 The sinus venosus defect is frequently associated with an abnormal connection of one or all of the right pulmonary veins.
The sinus venosus defect is frequently associated with an abnormal connection of one or all of the right pulmonary veins.
 Echocardiography is the method of choice for the diagnosis of atrial septal defect.
Echocardiography is the method of choice for the diagnosis of atrial septal defect.
 The chest radiograph characteristically shows dilatation of the central pulmonary arteries and an increase in diameter of the central and peripheral pulmonary vessels (Fig. 3.1).
The chest radiograph characteristically shows dilatation of the central pulmonary arteries and an increase in diameter of the central and peripheral pulmonary vessels (Fig. 3.1).
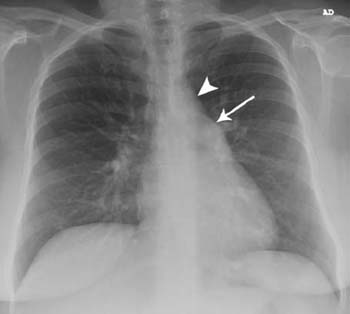
Fig. 3.1 Atrial septal defect in a 23-year-old woman. The heart size is normal; there is enlargement of the main pulmonary artery (arrow) and a small-appearing aortic arch (arrowhead). The pulmonary arteries centrally are mildly enlarged.
 Ventricular Septal Defect
Ventricular Septal Defect
 Ventricular septal defects are the most common congenital heart condition in infants and children.
Ventricular septal defects are the most common congenital heart condition in infants and children.
 Of these defects, 70% are located in the membranous portion of the interventricular septum, 20% in the muscular portion of the septum, 5% just below the aortic valve, and 5% near the junction of the mitral and tricuspid valves with associated atrioventricular canal defects.
Of these defects, 70% are located in the membranous portion of the interventricular septum, 20% in the muscular portion of the septum, 5% just below the aortic valve, and 5% near the junction of the mitral and tricuspid valves with associated atrioventricular canal defects.
 Individuals with a large defect may progress to heart failure as babies (Fig. 3.2); those who survive until adulthood usually have pulmonary hypertension with subsequent right ventricular hypertrophy and dilatation.
Individuals with a large defect may progress to heart failure as babies (Fig. 3.2); those who survive until adulthood usually have pulmonary hypertension with subsequent right ventricular hypertrophy and dilatation.
 Ventricular septal defects are frequently associated with complex congenital heart disease.
Ventricular septal defects are frequently associated with complex congenital heart disease.
 The chest radiograph may demonstrate a normal heart size or cardiomegaly. The pulmonary arteries show dilatation of the central vessels and an increase in diameter of the peripheral pulmonary vessels (Fig. 3.3).
The chest radiograph may demonstrate a normal heart size or cardiomegaly. The pulmonary arteries show dilatation of the central vessels and an increase in diameter of the peripheral pulmonary vessels (Fig. 3.3).
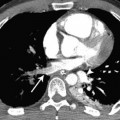
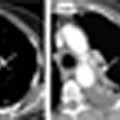
 Cross-sectional imaging demonstrates the primary defect and associated defects (Fig. 3.4).
Cross-sectional imaging demonstrates the primary defect and associated defects (Fig. 3.4).

Fig. 3.2 Large ventricular septal defect in a 3-month-old boy. Chest radiograph shows cardiomegaly, prominent enlarged pulmonary vessels, and perihilar consolidation, consistent with alveolar pulmonary edema.

Fig. 3.3 Ventricular septal defect with infundibular stenosis of the right ventricular outflow tract in a 24-year-old man. The heart is enlarged. The pulmonary arteries centrally and peripherally are enlarged.
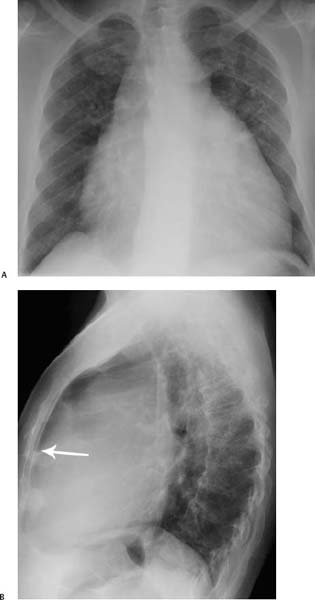

Fig. 3.4 (A–D) Ventricular septal defect in a 60-year-old man. (A) Chest radiograph shows that the heart is enlarged. The main, central, and peripheral pulmonary arteries are also enlarged. (B) Lateral radiograph shows dilatation of the right ventricle, evidenced by a decrease in the normal retrosternal translucency (arrow). Ventricular septal defect in a 60-year-old man. (C) CT demonstrates a large main pulmonary artery (PA). (D) A CT image obtained further caudad shows the ventricular septal defect (arrow).
 Patent Ductus Arteriosus
Patent Ductus Arteriosus
 In the fetus, the ductus arteriosus connects the left pulmonary artery with the descending aorta just distal to the left subclavian artery.
In the fetus, the ductus arteriosus connects the left pulmonary artery with the descending aorta just distal to the left subclavian artery.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


