29 Cardiomyopathies and Related Conditions
With Kevin S. Roman
Definition and Classification
 Traditionally, cardiomyopathies have been divided into primary and secondary forms. As the etiology of previously idiopathic disorders has been discovered, the distinction between primary and secondary forms has become increasingly tenuous. It has been proposed to define cardiomyopathy as a myocardial disorder in which the heart muscle is structurally and functionally abnormal, in the absence of known coronary artery disease, hypertension, valvular disease, and congenital heart disease sufficient to cause the observed myocardial abnormality.1
Traditionally, cardiomyopathies have been divided into primary and secondary forms. As the etiology of previously idiopathic disorders has been discovered, the distinction between primary and secondary forms has become increasingly tenuous. It has been proposed to define cardiomyopathy as a myocardial disorder in which the heart muscle is structurally and functionally abnormal, in the absence of known coronary artery disease, hypertension, valvular disease, and congenital heart disease sufficient to cause the observed myocardial abnormality.1
 Classification (Fig. 29.1)1:
Classification (Fig. 29.1)1:
- • Hypertrophic (HCM): presence of increased ventricular wall thickness or mass in the absence of loading conditions (hypertension, valve disease) sufficient to cause the observed abnormality
- • Dilated (DCM): presence of left ventricular dilatation and left ventricular systolic dysfunction in the absence of abnormal loading conditions (hypertension, valve disease) or coronary artery disease sufficient to cause global systolic impairment
- • Restrictive (RCM): restrictive ventricular physiology in the presence of normal or reduced diastolic volumes (of one or both ventricles), and normal or reduced systolic volumes
- • Arrhythmogenic right ventricular cardiomyopathy (ARVC): presence of right ventricular dysfunction (global or regional), with or without left ventricular disease, in the presence of histologic evidence for the disease or electrocardiographic abnormalities in accordance with published criteria
- • Unclassified:
- – Left ventricular noncompaction: presence of prominent left ventricular trabeculae and deep intertrabecular recesses
- – Takotsubo cardiomyopathy: presence of transient regional systolic dysfunction involving the left ventricular apex or midventricle in the absence of obstructive coronary disease on coronary angiography
 Each class is then subclassified into familial and nonfamilial forms.
Each class is then subclassified into familial and nonfamilial forms.
 Table 29.1
Table 29.1
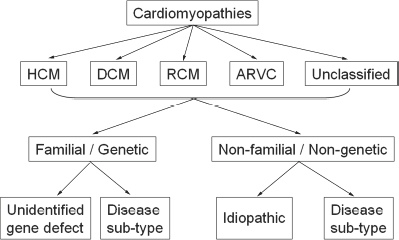
Fig. 29.1 Classification of cardiomyopathies.
Pathophysiology
 Hypertrophic cardiomyopathy
Hypertrophic cardiomyopathy
- • Rare form of cardiomyopathy in children
- • May be obstructive or nonobstructive depending on the pattern of myocardial hypertrophy
- • Myocardial hypertrophy develops in the absence of a hemodynamic afterload stress.
- • Hypertrophy causes decreased ventricular compliance and elevates end-diastolic pressure, resulting in diastolic dysfunction.
- • Ejection fraction and the rate of ejection are increased.
 Dilated cardiomyopathy
Dilated cardiomyopathy
- • Both end-systolic and end-diastolic volumes are increased, with decreased stroke volume and ejection fraction.
- • Mild to moderate atrioventricular valve regurgitation associated with ventricular dilation
- • Myocarditis refers to inflammation of the myocardium and may be due to either infectious organisms, most commonly viral, or noninfectious inflammatory conditions, such as systemic lupus erythematous, polyarteritis nodosa, and Kawasaki disease.
 Restrictive cardiomyopathy
Restrictive cardiomyopathy
- • Poor ventricular compliance with reduced diastolic filling
- • End-diastolic volume is usually normal or slightly reduced, and the ejection fraction is less than normal.
- • Loeffler’s disease is due to an immunologic reaction to the eosinophil, resulting in infiltration of the myocardium, thrombi in the ventricular cavities, and characteristic scarring of the posterior mitral valve leaflet.
 Arrhythmogenic right ventricular cardiomyopathy
Arrhythmogenic right ventricular cardiomyopathy
- • Desmosomal mutations causing detachment of myocytes and untimate; replacement of right ventricular myocardium with fibrous or adipose tissue causing arrhythmia of right ventricular origin
- • Right ventricular global or regional dysfunction