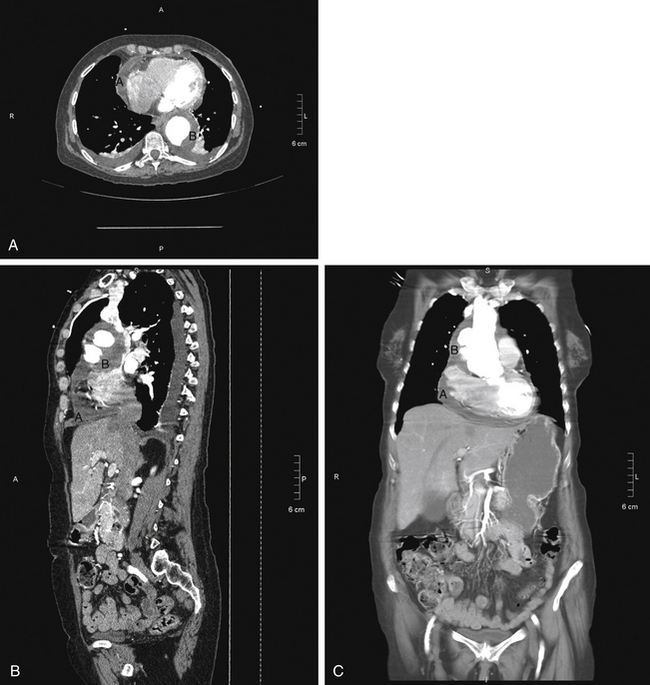
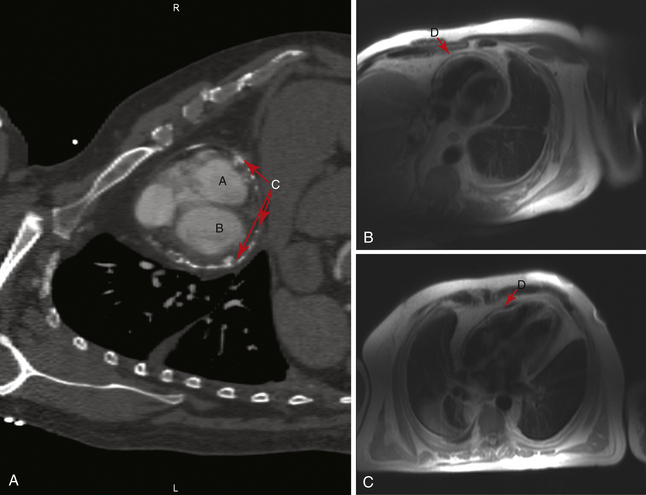
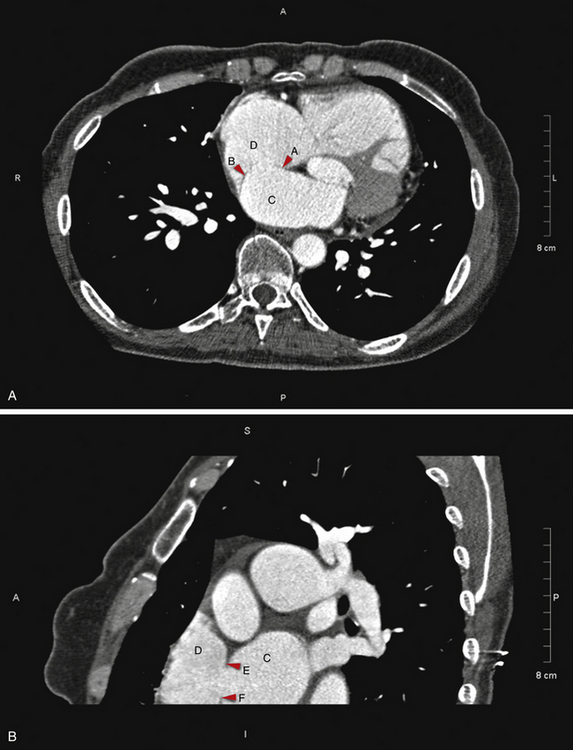
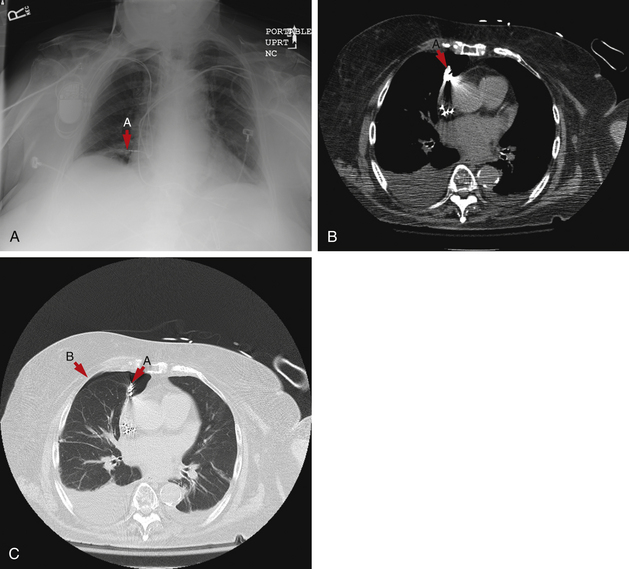
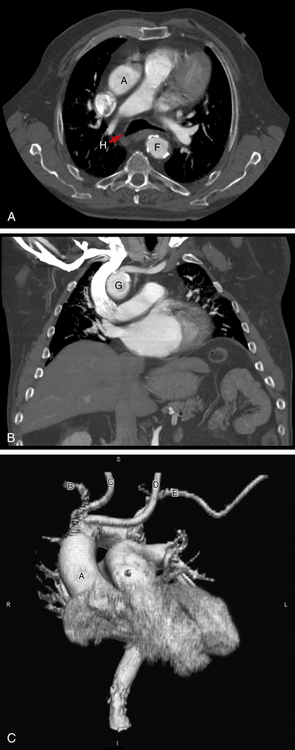
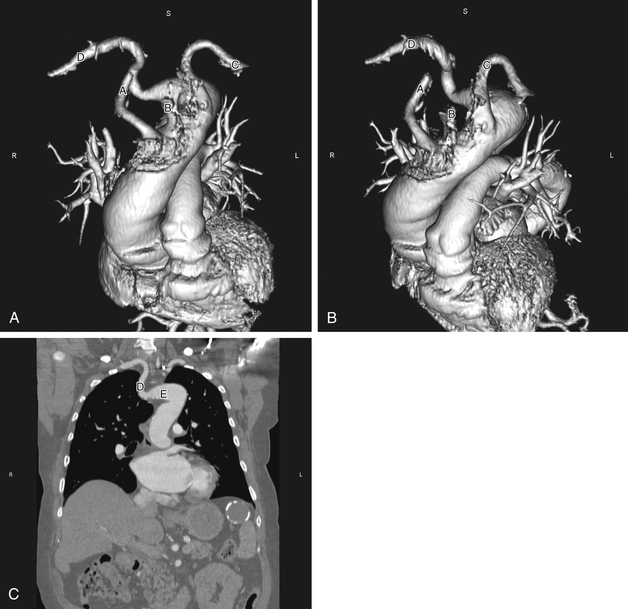
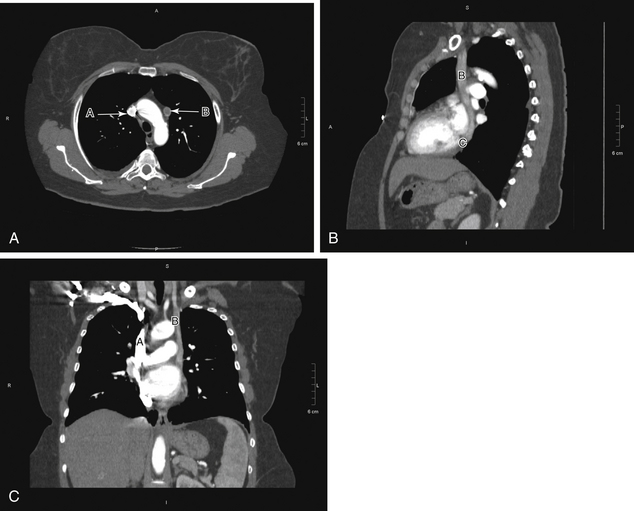
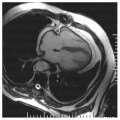
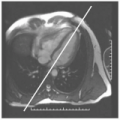
4 Cardiovascular Computed Tomography FIGURE 4-1 Pericardial effusion. Axial image from contrast-enhanced CT (A) with sagittal (B) and coronal (C) reconstructions. All of the images demonstrate moderate pericardial fluid (A). This fluid also extends superiorly around the great vessels and tracks inferior around the descending thoracic aorta (B). FIGURE 4-2 Pericarditis. A, A single short-axis postcontrast CT view of the heart demonstrates extensive calcification (C) of the pericardium adjacent to the right (A) and left (B) ventricles. Short-axis (B) and horizontal long-axis (C) postcontrast MRI views of the heart demonstrate enhancement of the pericardium (D), especially around the right ventricular wall. FIGURE 4-3 Atrial septal defect. A gated axial postcontrast-enhanced CT (A) with short-axis reconstruction (B) demonstrates a large ASD between the left (C) and right (D) atria. The residual anterior (A) and posterior (B) portions of the septum can be seen on the axial image. The short-axis image demonstrates the superior (E) and inferior (F) portions of the atrial septum. A gated cardiac MRI may demonstrate the direction of flow. FIGURE 4-4 Pacer lead perforation. Frontal chest x-ray (A) and axial noncontrast chest CT in mediastinal (B) and lung (C) windows. A, The chest x-ray demonstrates two sets of pacer leads with an atrial lead (A) that does not appear to be over the cardiac silhouette. B, Chest CT then clearly demonstrates that the atrial lead has perforated the anterior right atrial wall (A). C, The lung windows demonstrate a small anterior pneumothorax (B), not visible on the chest x-ray. FIGURE 4-5 Right-sided arch. Axial postcontrast-enhanced CT (A) with MIP coronal reconstruction (B) and a 3D view (C). A right-sided ascending aorta (A) is seen with a right-sided aortic arch (G) that passes posterior to the esophagus and trachea (H). Aberrant origin of the right carotid artery (C) is present but is not well visualized on this exam. The right subclavian (B) and left carotid (D) arteries are grossly unremarkable. The origin of the left subclavian artery (E) is more distal arising from the aortic arch. The aorta descends on the left side of the spine (F). FIGURE 4-6 Anomalous great vessels. Contrast-enhanced CT with 3D MIP views (A and B) and coronal reconstruction (C). The anomalous order of great vessels as they originate from the aortic arch is right carotid artery (A), left carotid artery (B), left subclavian artery (C), and finally right subclavian artery (D). The anomalous right subclavian artery passes behind the esophagus. The dilated origin of the right subclavian artery is called the diverticulum of Kommerell (E). FIGURE 4-7 Persistent left SVC. Axial contrast-enhanced CT (A) with sagittal (B) and coronal (C) reconstructions. A, The axial image shows a densely contrast filled right SVC (A) with less dense contrast in the left SVC (B). B and C, Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related posts: Cardiovascular Magnetic Resonance Imaging Echocardiography Angiography Electrocardiography Cardiovascular Magnetic Resonance Imaging Positioning Complete Protocol Example Stay updated, free articles. Join our Telegram channel Join Tags: Cardiovascular Imaging Review Expert Consult Dec 26, 2015 | Posted by admin in CARDIOVASCULAR IMAGING | Comments Off on Cardiovascular Computed Tomography Full access? Get Clinical Tree
4 Cardiovascular Computed Tomography FIGURE 4-1 Pericardial effusion. Axial image from contrast-enhanced CT (A) with sagittal (B) and coronal (C) reconstructions. All of the images demonstrate moderate pericardial fluid (A). This fluid also extends superiorly around the great vessels and tracks inferior around the descending thoracic aorta (B). FIGURE 4-2 Pericarditis. A, A single short-axis postcontrast CT view of the heart demonstrates extensive calcification (C) of the pericardium adjacent to the right (A) and left (B) ventricles. Short-axis (B) and horizontal long-axis (C) postcontrast MRI views of the heart demonstrate enhancement of the pericardium (D), especially around the right ventricular wall. FIGURE 4-3 Atrial septal defect. A gated axial postcontrast-enhanced CT (A) with short-axis reconstruction (B) demonstrates a large ASD between the left (C) and right (D) atria. The residual anterior (A) and posterior (B) portions of the septum can be seen on the axial image. The short-axis image demonstrates the superior (E) and inferior (F) portions of the atrial septum. A gated cardiac MRI may demonstrate the direction of flow. FIGURE 4-4 Pacer lead perforation. Frontal chest x-ray (A) and axial noncontrast chest CT in mediastinal (B) and lung (C) windows. A, The chest x-ray demonstrates two sets of pacer leads with an atrial lead (A) that does not appear to be over the cardiac silhouette. B, Chest CT then clearly demonstrates that the atrial lead has perforated the anterior right atrial wall (A). C, The lung windows demonstrate a small anterior pneumothorax (B), not visible on the chest x-ray. FIGURE 4-5 Right-sided arch. Axial postcontrast-enhanced CT (A) with MIP coronal reconstruction (B) and a 3D view (C). A right-sided ascending aorta (A) is seen with a right-sided aortic arch (G) that passes posterior to the esophagus and trachea (H). Aberrant origin of the right carotid artery (C) is present but is not well visualized on this exam. The right subclavian (B) and left carotid (D) arteries are grossly unremarkable. The origin of the left subclavian artery (E) is more distal arising from the aortic arch. The aorta descends on the left side of the spine (F). FIGURE 4-6 Anomalous great vessels. Contrast-enhanced CT with 3D MIP views (A and B) and coronal reconstruction (C). The anomalous order of great vessels as they originate from the aortic arch is right carotid artery (A), left carotid artery (B), left subclavian artery (C), and finally right subclavian artery (D). The anomalous right subclavian artery passes behind the esophagus. The dilated origin of the right subclavian artery is called the diverticulum of Kommerell (E). FIGURE 4-7 Persistent left SVC. Axial contrast-enhanced CT (A) with sagittal (B) and coronal (C) reconstructions. A, The axial image shows a densely contrast filled right SVC (A) with less dense contrast in the left SVC (B). B and C, Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related posts: Cardiovascular Magnetic Resonance Imaging Echocardiography Angiography Electrocardiography Cardiovascular Magnetic Resonance Imaging Positioning Complete Protocol Example Stay updated, free articles. Join our Telegram channel Join Tags: Cardiovascular Imaging Review Expert Consult Dec 26, 2015 | Posted by admin in CARDIOVASCULAR IMAGING | Comments Off on Cardiovascular Computed Tomography Full access? Get Clinical Tree