Complete Protocol Example
Mark Doyle
OUTLINE
For the fictitious “XYZ Trial”, we will discuss how the required views and features of the cardiovascular magnetic resonance (CMR) protocol should be obtained. In the XYZ Trial, the main information to be obtained concerns cardiac function. We will point out some efficiency notes including features to be aware of and approaches to overcome some commonly encountered difficulties.
GENERAL CARDIOVASCULAR MAGNETIC RESONANCE REQUIREMENTS AND CARDIAC VIEWS
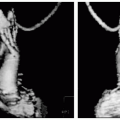
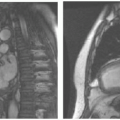
In the XYZ Trial, CMR data are to be used to evaluate patients for entry into the trial. The CMR data requested may differ substantially from your normal diagnostic protocol, and special attention should be paid to the required elements of each scan. For study completeness, it is essential that views contain the correct landmark information. The fictitious XYZ Trial requires four data sets (see Fig. 35-1), along with blood pressure measurements:
Long axis two-chamber cine
Long axis four-chamber cine
Multislice short axis cine series
Phase contrast velocity scans of aortic outflow
Some details of the key scans to be obtained are outlined in the Table 35-1.
To obtain the key scans, additional planning scans are also required. Planning scans occupy time, as does the positioning of target scans. This overhead has to be accommodated when budgeting time to perform the protocol, as should activities such as patient preparation, establishing the electrocardiogram (ECG) signal, obtaining blood pressures, and transmission of data.
PATIENT PREPARATION
After normal patient screening and precautions have been observed, position the patient on the scanner table (typically feet first). Connect ECG leads, respiratory gating device, and blood pressure cuff. The XYZ Trial protocol requires that blood pressure be monitored at the time of the CMR examination. Ideally, this information should be acquired at 2-minute intervals throughout the CMR examination. Manually record the end-systolic, end-diastolic, mean blood pressure and the time at which they were measured. Once the patient is positioned on the scanner table and a strong ECG signal is established, “center” on the midline of the chest, approximately 8 cm (3 in.) above the zyphoid notch.
PLAN SCAN GUIDELINES
Plan all scans using the end-diastolic cardiac phase to ensure that the heart is seen in its maximally extended condition. Wherever possible, use ECG triggered scans to plan views. If a view does not contain the required features, consider repeating the scan and/or repeating the scout scan from which it was planned. If image quality is suboptimal, consider remedial action before proceeding. Note that ECG and respiratory-related issues are responsible for most quality issues and that problematic scans that are used for planning further views usually compound problems further into the study.
SCAN PHILOSOPHY
Acquire scans in a progressive order such that planning of the next scan relies on the previously acquired scan. Do not proceed to the next step until you are satisfied
that the previous scan data has been adequately acquired.
that the previous scan data has been adequately acquired.
 FIGURE 35-1 The four key views to be obtained for the fictitious XYZ Trial are shown (top-left and clockwise): two-chamber cine, four-chamber cine, phase contrast cine, and short axis cine. |
SCOUT IMAGING
Obtain a non-cardiac triggered scout image-set. A typical set consists of three sets of orthogonal scans:
Seven slices transverse
Seven slices sagittal
Seven slices coronal
Non-ECG triggered scouts are generally of too low a quality to allow for detailed planning purposes. For this reason, acquire an ECG triggered set of scout images. Typical parameters are:
256 × 128 matrix
TABLE 35-1 Key scan details | |||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Plan a set of approximately eight transverse slices centered through the heart from a coronal scan. Perform the scans under breath-hold conditions, or conditions similar to those to be used for the cine images to be obtained later.
BREATH-HOLDING GUIDELINES
During breath-holding, it is important to note that the heart may be in a different position compared to normal breathing. When planning breath-hold scans, more reproducible results are achieved when planning them using scans obtained under the same breath-hold strategy. For consistency in breath-hold position and to maximize compliance, the following instructions may be given to the patient after all “prep” scan procedures are complete and the scan is ready to proceed:
“Take a deep breath in”
“Leave it out half way”
“Do not breathe” (start scan)
Upon scan completion, instruct patient to breathe. If a patient experiences difficulty in performing breath-holding, consider administering oxygen:
2 L per minute
Titrating O2 saturation up to 90%
CARDIOVASCULAR MAGNETIC RESONANCE CINE FEATURES
All of the key scans to be obtained are cines, that is, cardiac triggered, showing movie information throughout the cardiac cycle. Exact details of performing cine scans will typically vary from site to site. In the XYZ Trial, general guidelines are given describing details of the cine imaging technique. All cine scans should be cardiac triggered. If possible, perform cine scanning using a breath-hold method. If breath-holding is not feasible, use respiratory compensation and/or respiratory gating/triggering. The SSFP




Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
