Two medical students spotted a bear while walking in the woods. Student 1 took out sneakers from his backpack and put them on. “You can’t outrun a bear,” said Student 2. Said Student 1, “I don’t have to. I just have to outrun you.” |
- 1
Figure 12-1A shows how the heart sits in the chest. Figure 12-1B , we look at the heart and great vessels. On the left side, there are four bulges (moguls to you skiers). They are:
|
- 1
1. E. aortic arch
- 2.
F. main pulmonary artery
- 4.
C. left ventricle
|
- 1.
_____________
- 2.
_____________
- 3.
left atrial appendage
- 4.
_____________
|
- A.
superior vena cava
- B.
left atrium
- C.
left ventricle
- D.
descending aorta
- E.
aortic arch
- F.
main pulmonary artery
|
Note: The normal left atrial appendage is flat or concave, not convex. |
- 2
The right heart border is formed by the right atrium (5) . The right ventricle does not usually form a lateral border on the frontal view.
|
|
- 5.
right atrium
- 6.
_____________
- 7.
_____________
|
- A.
ascending aorta
- B.
aortic arch
- C.
thymus
- D.
superior vena cava
- E.
thyroid
|
- 3
On the lateral film, the right heart is anterior, and the left heart is posterior. Test yourself by labeling the cardiovascular structures on the lateral ( Figure 12-1C ).
|
- 3
1. F. aortic arch
- 3.
A. left atrium
- 4.
B. left ventricle
- 6.
E. ascending aorta
- 8.
D. right ventricle
- 9.
G. descending aorta (proximal)
|
- 1.
_____________
- 3.
_____________
- 4.
_____________
- 6.
_____________
- 8.
_____________
- 9.
_____________
|
- A.
left atrium
- B.
left ventricle
- C.
right atrium
- D.
right ventricle
- E.
ascending aorta
- F.
aortic arch
- G.
descending aorta (proximal)
- H.
superior vena cava
|
When reading images, forget about “right heart/left heart.” Think “anterior heart/posterior heart.” In reality, the right heart is anterior and the left heart is posterior—not left and right. |
- 4
Sometimes the terminology is confusing. Review the following:
|
|
The left heart sits _____________ to the right heart.
|
|
On the frontal view, the normal right heart border is formed by the _____________ only.
- A.
right atrium
- B.
right ventricle
- C.
both A and B
- D.
ascending aorta
|
|
On the frontal view, the left atrial appendage is normally _____________ and _____________.
- A.
concave
- B.
convex
- C.
above the pulmonary artery
- D.
below the pulmonary artery
|
- A.
concave
- D.
below the pulmonary artery
|
- 5
Test yourself on Figure 12-1D by identifying the following:
|
- 5
a. right ventricle
- b.
right atrium
- c.
left ventricle
- d.
left atrium
- e.
pulmonary vein
- f.
descending aorta
- ←
pericardium
|
- a.
_____________
- b.
_____________
- c.
_____________
- d.
_____________
- e.
_____________
- f.
_____________
- ←
_____________
|
ascending aorta
descending aorta
right atrium
left atrium
right ventricle
left ventricle
pericardium
pulmonary artery
|
Note how the right atrium forms the right heart border and the right heart is anterior. |
|
Determining cardiac enlargement is easy. Measure the horizontal width of the heart and divide it by the widest internal diameter of the thorax. The normal cardiothoracic ratio is less than 0.5. (This is oversimplified, but useful.) |
- 6
In Figure 12-2 , the cardiothoracic ratio is 0.43.
|
|
The upper limit of normal is _____________.
- A.
42%
- B.
45%
- C.
50%
- D.
55%
|
|
These measurements are unreliable on an anteroposterior image because of _____________.
- A.
cardiac magnification
- B.
edge unsharpness
- C.
the heart is closer to the film
- D.
grid effect
|
|
CLINICAL PEARL: The cardiothoracic ratio is based on population standards. For a given patient, an increase of greater than 1 cm in cardiac diameter from a prior film is a more reliable index of cardiac enlargement than the cardiothoracic ratio. In general, a radiologist with a ruler is a radiologist in trouble, but these measurements work fairly well on erect, inspiratory posteroanterior (PA) radiographs. |
The “heart” may be enlarged because of intrinsic cardiac disease or appear enlarged by surrounding pericardial fluid. For this reason, many prefer the term cardiac silhouette to “heart size.” |
- 7
If the left atrium enlarges, it protrudes _____________ and _____________.
- A.
laterally
- B.
medially
- C.
anteriorly
- D.
posteriorly
- E.
inferiorly
|
|
On the frontal view, its margin becomes _____________.
|
|
Figures 12-3A and 12-3B show an enlarged left atrium. The upper left heart border bulges laterally ( arrow on Figure 12-3A ) and posteriorly ( arrow on Figure 12-3B ). Compare with Figures 12-1A and 12-1B . |
- 8
In Figures 12-4A and 12-4B , test yourself by identifying the following:
|
- 8
1. B. left ventricle
- 2.
D. descending aorta
- 3.
C. ascending aorta
|
- 1.
white arrow
- 2.
black arrowhead
- 3.
white arrowhead
|
- A.
left atrium
- B.
left ventricle
- C.
ascending aorta
- D.
descending aorta
- E.
right atrium
- F.
superior vena cava
|
The aorta is so tortuous that even the aortic arch is visible on the lateral. |
|
- 9
From Figure 12-4A and 12-4B , left ventricular enlargement displaces the border _____________ and _____________.
- A.
anteriorly
- B.
posteriorly
- C.
superiorly
- D.
inferiorly
- E.
medially
- F.
laterally
|
|
- 10
To review: A large left atrium bulges _____________ on the PA film and _____________ on the lateral film.
- A.
anteriorly
- B.
posteriorly
- C.
laterally
- D.
medially
- E.
inferiorly
- F.
superiorly
|
|
A large left ventricle bulges _____________ on the PA and _____________ on the lateral x-rays.
- A.
anteriorly
- B.
posteriorly
- C.
laterally
- D.
medially
- E.
inferiorly
- F.
superiorly
|
- C.
laterally
- B.
posteriorly
|
Detecting right heart enlargement is more difficult. In the frontal projection, the normal right heart protrudes slightly to the right of the spine, and an enlarged right heart protrudes further to the right (soft science, at best). In the lateral projection, the right heart enlarges anteriorly and superiorly. The normal right heart contacts the lower one third of the sternum, whereas the enlarged right heart contacts the lower one half. Compare the enlarged right heart ( Figures 12-5A and 12-5B ) with the enlarged left heart in Figures12-4A and 12-4B . |
- 11
Many heart diseases also alter the pulmonary vessels.
|
|
In a normal erect patient, gravity causes most blood to flow to the _____________.
- A.
apex
- B.
base
- C.
anterior
- D.
posterior
|
|
In a supine patient, the blood flow _____________.
- A.
evens out
- B.
is greater in the upper than the lower lobes
- C.
is similar to erect position
|
- A.
evens out (although more flows posteriorly)
|
- 12
Compare chest PA images in Figures 12-6A and 12-6B . The upper lobe vessels are smaller in _____________.
|
|
The upper lobe vessels are sharper and better defined in _____________.
|
|
Figure 12-6A is normal. In Figure 12-6B , the upper lobe vessels are bigger and their edges less distinct. This is called cephalization or vascular redistribution. Cephalization, not heart size, is the key to diagnosing elevated left heart pressure. Compare Figure 12-6A and Figure 12-6B until cephalization is absolutely clear. |
|
CLINICAL PEARL: Left heart failure and mitral valve stenosis are the most frequent causes of redistribution or cephalization. A shunt (e.g., atrial or ventricular septal defect) causes all vessels to enlarge due to chronic high blood flow. |
- 13
Look at Figures 12-7A and 12-7B .
|
|
Which patient has prominent upper lobe vessels as a result of an atrial septal defect?
|
|
- 14
As the left atrial pressure increases, interstitial edema develops.
|
|
The interstitial edema causes the vessel margins to become _____________.
|
|
The peripheral interstitial markings become _____________ prominent.
|
|
- 15
In left heart failure, the cardiac silhouette often enlarges. In addition:
|
|
In mild failure, there is _____________ of the vessels but no edema.
- A.
cephalization
- B.
generalized enlargement
- C.
no change
- D.
cardiomegaly
|
|
Moderate failure causes indistinct vessel margins as a result of _____________ edema.
- A.
alveolar
- B.
interstitial
- C.
magnification
|
|
Severe failure causes _____________ edema and pleural effusions.
- A.
alveolar
- B.
interstitial
|
|
- 16
Figure 12-8 shows four phases of left heart failure. Match the images with the descriptions.
|
- 16
1. normal
- 2.
alveolar edema
- 3.
interstitial edema
- 4.
vascular congestion
|
|
alveolar edema
interstitial edema
vascular congestion
normal
|
Edema tends to be bilateral and favors the mid and lower lungs. |
|
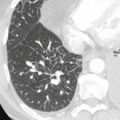
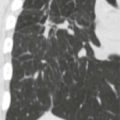
When fluid enters the interstitium, it swells. It often makes the interlobular septa visible. These are called Kerley lines. On the chest x-ray ( Figure 12-9A ) they are small lines perpendicular to the pleura ( arrows ). They are easy to see on computed tomography (CT) ( Figure 12-9B ). |
CLINICAL PEARL: With vessel cephalization alone, lung auscultation is usually normal. With interstitial edema, crackling rales are audible. With alveolar edema, rales are audible. |
- 17
Figure 12-10 is a portable radiograph.
|
|
It is taken _____________.
|
- A.
supine ( arrow points down)
|
The cardiothoracic ratio is _____________.
- A.
>50%
- B.
<50%
- C.
not valid
|
- C.
not valid (magnification)
|
The upper lobe pulmonary vessels are _____________.
- A.
prominent
- B.
normal
- C.
not valid
|
- C.
not valid (vessels are often prominent in normal supine patients.)
|
Is the patient in heart failure?
- A.
yes
- B.
no
- C.
can’t tell
|
|
Determining cardiomegaly and cephalization is unreliable on supine films. |
- 18
Name the physiologist whose law described the relationship between edema, hydrostatic pressure, and oncotic pressure: _____________.
|
|
Figure 12-11 is a _____________.
|
|
- 19
Figure 12-12A is a PA radiograph:
|
|
Cardiothoracic ratio is _____________.
|
|
|
|
|
|
Is there a pleural effusion?
|
|
Figure 12-12B , an echocardiogram, shows a large pericardial effusion (P). |
|
Figure 12-13 , a CT scan of a different patient, shows a pericardial effusion (p). The heart is not enlarged. There are bilateral pleural effusions and left lower lobe consolidation (atelectasis). Echocardiography, CT, and magnetic resonance imaging accurately depict pericardial effusions, but echocardiology is most cost-effective. |
CLINICAL PEARL: Marked generalized enlargement of the cardiac silhouette, with no or mild signs of left heart failure, is most likely due to pericardial effusion. Cardiomyopathy and multivalvular heart disease may have a similar radiographic presentation. |