Cartilage-Forming (Chondrogenic) Lesions
Diagnosis of a bone lesion as originating from cartilage is usually a simple task for the radiologist. The lesion’s radiolucent matrix, scalloped margin, and punctate, annular, or comma-shaped calcifications usually suffice to establish its chondrogenic nature. Yet determination if a cartilage tumor is benign or malignant, often creates a problem for the radiologist and even for the pathologist. All cartilage tumors, regardless if benign or malignant, exhibit a positive reaction for S-100 protein, a helpful diagnostic hint. Histologically, cartilaginous lesions are usually recognized by the features of their intercellular matrix, which has a uniformly translucent appearance and contains less collagen than do the bone-forming tumors. The tumor cells are located in rounded spaces, called lacunae, as in normal cartilage. In benign cartilage tumors, like enchondroma, the tissue is sparsely cellular. The cells usually contain small darkly stained nuclei. The tumor tissue is avascular, and areas of calcified matrix are common. Because of their slow growth, enchondromas expand into the endocortex creating small erosions (scalloping). Conversely, chondrosarcomas exhibit pleomorphism, large nuclei, double nuclei, and mitoses. These tumors invade the endocortex, form deep scalloping, and are associated with cortical thickening, periosteal reaction, and not infrequently a softtissue mass.
A. BENIGN CARTILAGE-FORMING LESIONS
Enchondroma
Definition:
Benign hyaline cartilage neoplasm arising in the medullary portion of bone.
Epidemiology:
Ten to twenty-five percent of all benign bone tumors.
Age range from 5 to 80 years.
Most common in the second through fourth decades of life.
Solitary enchondromas are rare in young children, whereas multiple enchondromas are encountered more commonly.
Both genders are equally affected.
Sites of Involvement:
Any bone formed by endochondral ossification can be affected.
Common in the short tubular bones (phalanges and metacarpals) of the hands, followed by bones of the feet, and the long bones, especially proximal humerus and proximal and distal femur.
In the long bones, the tumors are usually centrally located within metaphysis or diaphysis.
Epiphyseal involvement is rare.
Clinical Findings:
In the small bones of the hands and feet typically presents as palpable swellings, with or without pain.
Common expansion of small bones and attenuation of the cortex may cause pathologic fractures, which may resemble aggressive malignant behavior.
In the long bone, tumors are more often asymptomatic and are detected incidentally in the imaging studies obtained for other reasons.
Imaging:
Radiography shows well-marginated lesion that vary from radiolucent to heavily mineralized (calcified) (Figs. 3.1 and 3.2).
Cortex is usually thinned out and expanded in symmetric fusiform fashion.
Calcification pattern is characteristic, consisting of punctate (stippled), flocculent, or curvilinear (in form of ring, comma-shaped, and arc pattern) calcifications, exhibiting “popcorn”-like appearance (see Figs. 1.6C, 1.17, 1.18A, and 3.2).
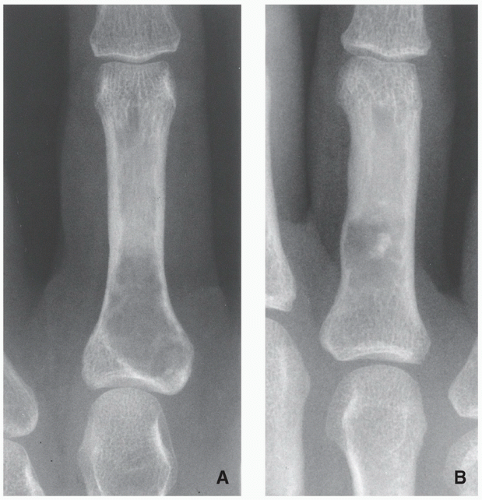
FIGURE 3.1 Radiography of enchondroma. (A) Radiolucent lesion in the proximal phalanx of the middle finger of a 40-yearold woman and (B) a similar lesion with central calcification in the proximal phalanx of the ring finger of a 42-year-old man are typical examples of enchondroma in the short tubular bones.
Lesions in the small tubular bones can be centrally or eccentrically located, and larger tumors may completely replace medullary cavity.
Occasionally, intracortical lesions are present, resembling osteochondromas (see Fig. 3.12).
Shallow endosteal scalloping is usually present (see Fig. 3.2C).
There is no periosteal reaction, unless pathologic fracture has occurred.
Cortical destruction and soft-tissue invasion should never be seen in enchondromas and would be most consistent with chondrosarcoma.
Skeletal scintigraphy shows mildly increased uptake of radiopharmaceutical agent in uncomplicated lesions, whereas the presence of a pathologic fracture or malignant transformation is revealed by marked scintigraphic activity.
Computed tomography further delineates the tumor and more precisely localizes it in the bone; it shows to better advantage the scalloped borders and matrix calcifications.
Magnetic resonance imaging—T1-weighted sequences show the lesion to be of low-to-intermediate signal intensity, whereas on T2-weighted and other watersensitive sequences, the lesions will exhibit high signal, with calcifications imaged as low signal intensity structures (Figs. 3.3 and 3.4). After intravenous administration of gadolinium, there is enhancement of the lesion (Figs. 3.5D and 3.6C).
Pathology:
Gross (Macroscopy):
Most enchondromas measure less than 3 cm in length, and tumors larger than 5 cm are uncommon.
Cartilaginous multinodular architecture is separated by bone marrow.
Multinodular pattern is seen more often in long bones compared to confluent growth pattern in small tubular bones.
Histopathology:
Cartilage nodules may cause shallow impressions on endocortex, but no invasion is present (Fig. 3.7).
Cartilage nodules frequently undergo endochondral ossification (Fig. 3.8).
Cartilage shows low-to-moderate cellularity and contains chondrocytes of variable size located in the lacunae, exhibiting small, round, and hyperchromatic nuclei (Figs. 3.9A,B and 3.10B).
Occasionally, scattered binucleated cells are present (Fig. 3.9C).
Nodules of hyaline cartilage are well demarcated by the surrounding bone and bone marrow (Fig. 3.10A).
Calcifications may be present.
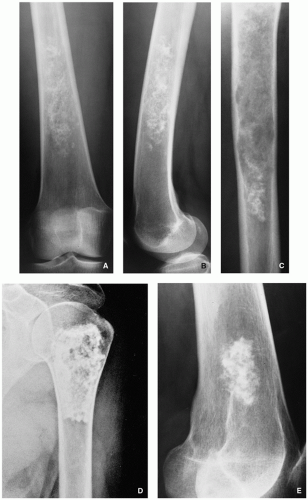 FIGURE 3.2 Radiography of enchondroma. (A) Anteroposterior and (B) lateral radiographs of the femur show a radiolucent lesion with “popcorn”-like calcifications. (C) In another patient, a radiolucent lesion in a long tubular bone exhibits central calcifications and shallow scalloping of the endocortex reflecting the lobular growth pattern of cartilage. At the site of the lesion, the cortex is thin-out. (D) A heavily calcified lesion (so-called calcifying enchondroma) is seen in the proximal humerus of a 58-year-old woman. Note that despite of the large size of the lesion, the cortex is not thickened. (E) Another lesion with typical stippled and annular calcification is present in the distal femur of a 30-year-old man. |
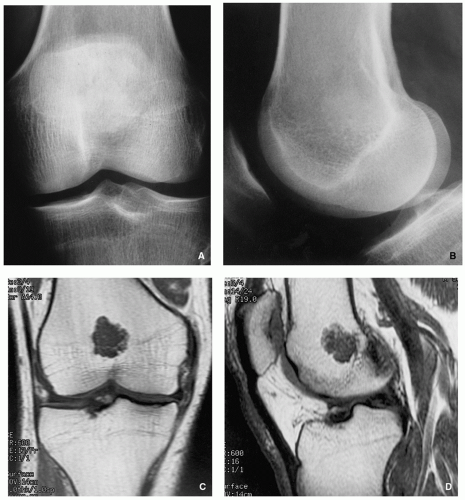 FIGURE 3.3 Radiography and magnetic resonance imaging of enchondroma. (A) Anteroposterior and (B) lateral radiographs of the left knee show an almost nondiscernible lesion in the distal femur. (C) Coronal and (D) sagittal T1-weighted MR images reveal the full extent of the tumor. |
Genetics:
Structural abnormalities involving chromosomes or chromosomal regions 4q, 7, 11, 14q, 16q22-q24, 20, and particularly rearrangement of chromosome 6 and 12q12-q15.
Complications:
Pathologic fracture.
Malignant transformation.
Prognosis:
Solitary enchondromas are successfully treated by intralesional curettage in most cases, and local recurrences are uncommon.
Differential Diagnosis:
▪ Medullary bone infarct
Well-defined, sclerotic, serpentine border.
Lack of endosteal scalloping.
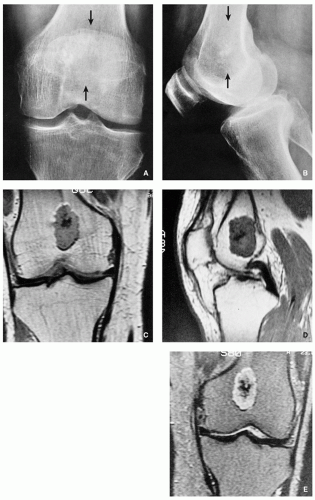 FIGURE 3.4 Radiography and magnetic resonance imaging of enchondroma. (A) Anteroposterior and (B) lateral radiographs of the knee of a 61-year-old man show a few calcifications in the distal femur (arrows). The nature and extent of the lesion cannot be adequately determined. (C) Coronal and (D) sagittal T1-weighted MR images demonstrate a well-circumscribed, lobulated lesion exhibiting intermediate signal intensity. The low signal intensity areas in the center represent calcifications. (E) Coronal T2-weighted MR image shows the lesion displaying a high intensity signal, with calcifications remaining of low signal. |
 FIGURE 3.5 Radiography and magnetic resonance imaging of enchondroma. (A) Anteroposterior and (B) axillary radiographs of the right shoulder of a 52-year-old man show a radiolucent lesion in the proximal humerus with chondroid type of calcifications. Note that despite the size of the lesion that extends from the lateral to medial cortex, there is no endosteal scalloping and the cortex is not thickened, the typical signs of benignity. (C) Coronal inversion recovery MRI and (D) sagittal T1-weighted fat-suppressed contrast-enhanced MR image confirm that the lesion is entirely within the medullary portion of the bone. The cortex is intact, there is no periosteal reaction, and there is lack of soft-tissue extension. |
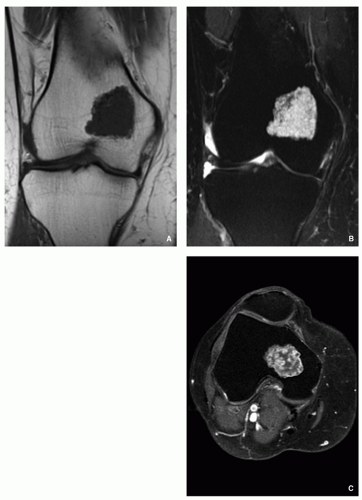 FIGURE 3.6 Magnetic resonance imaging of enchondroma. (A) Coronal T1-weighted MR image of the right knee of a 59-year-old woman shows a sharply demarcated lesion in the medial femoral condyle displaying low signal intensity. (B) Coronal T2-weighted MR image shows the lesion exhibiting high signal intensity with a few low signal foci, representing calcifications. (C) Axial T1-weighted fat-suppressed MRI obtained after intravenous administration of gadolinium shows significant enhancement of the tumor. Calcifications remain of low signal intensity. |
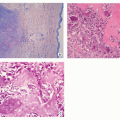
 FIGURE 3.7 Histopathology of enchondroma. (A) Whole-mount section (H&E) shows the tumor consisting of cartilaginous lobules and extends from the medial to the lateral cortex of the femur causing shallow endosteal scalloping. (B) On the higher magnification, there is no evidence of invasion, only shallow pressure/erosion of the endocortex (H&E, original magnification ×183). |
MRI (water-sensitive sequences) shows characteristic double-line signal intensity pattern.
▪ Low-grade chondrosarcoma
Length of the lesion greater than 5 cm.
Thickening of the cortex.
Deep endosteal scalloping.
Histopathology shows increased cellularity, cytologic atypia, hyperchromasia of the nuclei and binucleasion, and occasionally stromal myxoid changes.
Permeation and entrapment of bone trabeculae.
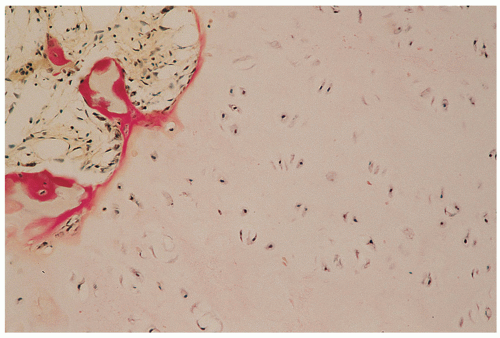 FIGURE 3.8 Histopathology of enchondroma. Cartilage lobules are surrounded by a narrow rim of bone, representing endochondral ossification (H&E, original magnification ×250). |
Enchondromatosis, Ollier Disease, and Maffucci Syndrome
Enchondromatosis—two or more enchondromas not associated with bone deformities or growth disturbance (Figs. 3.11 and 3.12).
Ollier disease (nonhereditary disorder)—multiple enchondromas with strong preference for one side of the body (monomelic distribution), associated with bone growth disturbance (Figs. 3.13, 3.14, 3.15 and 3.16).
Maffucci syndrome (nonhereditary disorder)—Ollier disease associated with hemangiomas of soft tissue (Figs. 3.17 and 3.18).
Clinical features of both conditions are knobby swelling of the digits and gross disparity in the length of the forearms and legs.
Clinical behavior of these conditions is unpredictable, and there is no specific treatment.
Most serious complication is malignant transformation of an enchondroma in Ollier disease (25% to 30% of affected patients) and Maffucci syndrome (greater than 50%) (see Fig. 3.18).
Patients with these conditions must have lifetime monitoring of their tumors.
Histologically, the enchondromas of these entities are similar to those of sporadic solitary tumors; however, they frequently demonstrate a greater degree of cellularity, demonstrate cytologic atypia, and may contain myxoid stroma, which may suggest the diagnosis of chondrosarcoma.
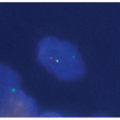
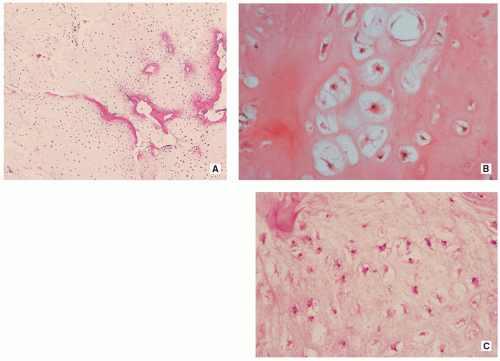 FIGURE 3.9 Histopathology of enchondroma. (A) Lowmagnification photomicrograph shows that the lesion consists of hyaline cartilage exhibiting low-to-moderate cellularity (H&E, original magnification ×50). (B) At higher magnification, the chondrocytes with darkly stained nuclei are seen to be located in the lacunae (H&E, original magnification ×100). (C) Occasionally binucleated cells may be present (H&E, original magnification ×150). |
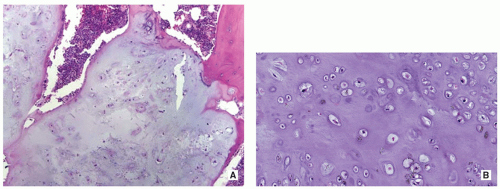 FIGURE 3.10 Histopathology of enchondroma. (A) Nodules of hyaline cartilage are well demarcated by the surrounding bone and bone marrow (H&E, original magnification ×50). (B) Higher-magnification photomicrograph shows low-to-moderate cellularity of the cartilage tissue containing chondrocytes of variable size located in the lacunae (H&E, original magnification ×200). |
 FIGURE 3.11 Radiography of enchondromatosis. Dorsovolar radiograph of the left hand of a 30-year-old woman shows several enchondromas affecting the fourth and fifth metacarpal bones, as well as the phalanges of the middle, ring, and small fingers. The remaining skeleton was not affected. |
Periosteal (Juxtacortical) Chondroma
Definition:
Benign cartilaginous lesion, almost identical to enchondroma, but growing on the surface of the bone in or beneath the periosteum.
Epidemiology:
Less than 2% of all benign cartilaginous lesions.
Most common in the second and third decades of life.
Children and adults are equally affected.
Sites of Involvement:
Long and short tubular bones with most common location in the proximal humerus.
Clinical Findings:
Common presentation as palpable, often painful mass.
Imaging:
Radiography shows cartilaginous lesion on the surface of the bone, with or without cortical erosion, that may contain calcifications, commonly associated with a buttress of periosteal reaction (Figs. 3.19 and 3.20); larger lesions resemble sessile osteochondromas (Fig. 3.21).

FIGURE 3.12 Radiography of enchondromatosis. In this 12-year-old boy, the intracortical lesion in the metaphysis of the forth metacarpal bone protrudes from the cortex (arrow), thus resembling an osteochondroma.
CT and MRI demonstrate separation of the lesion from the medullary portion of host bone (Figs. 3.21 and 3.22).
Pathology:
Gross (Macroscopy):
Well-marginated bone surface tumors.
Cortex underlying the tumor is usually thickened and may be eroded.
Most of the time, tumors are less than 6 cm in greatest diameter.
Histopathology:
Can be more cellular than enchondroma, occasionally cellular atypia is present (Fig. 3.23).
Prognostic Factors:
Recurrence rate is low after total excision.
Differential Diagnosis:
▪ Sessile osteochondroma
Continuity of the cortices of the lesion and host bone.
Continuity of the cancellous portions of the lesion and host bone.
 FIGURE 3.13 Radiography of Ollier disease. The classic features of this disorder in a 17-year-old boy are demonstrated in extensive involvement of multiple bones. (A) Anteroposterior radiograph of the pelvis shows crescent-shaped and ring-like calcifications in the tongues of cartilage extending from the iliac crests and proximal femora. (B) Anteroposterior radiograph of both legs shows growth stunting and deformities of the tibiae and fibulae. (C) In another patient, a 6-year-old boy, note extensive involvement of the distal femur and proximal tibia. |
 FIGURE 3.14 Radiography of Ollier disease. (A) Dorsovolar radiograph of the left hand of a 17-year-old girl shows extensive involvement of several metacarpals and phalanges by enchondromas. Note also involvement of the distal ulna, which in addition shows growth stunting, one of the features of this disorder. (B) Dorsovolar radiograph of the right hand of a 24-year-old woman shows extensive involvement of the metacarpals and phalanges by large expansive cartilaginous lesions. (C) Dorsovolar radiograph of the right hand of a 48-year-old man shows multiple enchondromas, some presenting as large lobulated cartilaginous masses of the phalanges. |
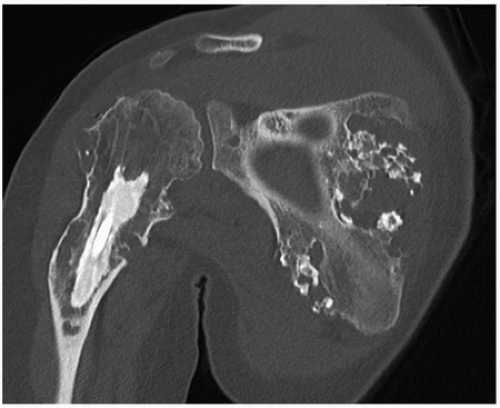 FIGURE 3.15 Computed tomography of Ollier disease. Coronal reformatted CT image of the right shoulder of a 23-year-old woman shows several enchondromas of different sizes affecting the proximal humerus and the scapula. |
 FIGURE 3.16 Magnetic resonance imaging of Ollier disease. (A) Anteroposterior radiograph of the right humerus of the same patient as depicted in Fig. 3.15 shows numerous enchondromas affecting proximal half of the bone. (B) Coronal T1-weighted MR image shows heterogeneous but predominantly low signal intensity of the lesions. |
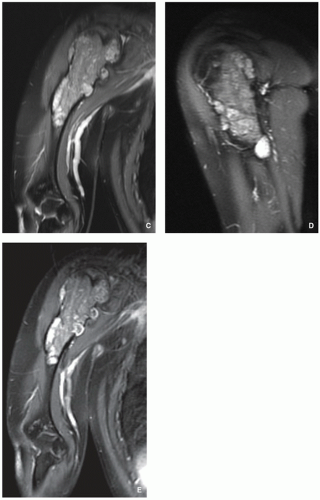 FIGURE 3.16 (Continued). (C) Coronal and (D) sagittal T2-weighted MR images show heterogeneous but predominantly high signal intensity of the lesions. (E) After intravenous administration of gadolinium, there is strong peripheral enhancement of multiple enchondromas. |
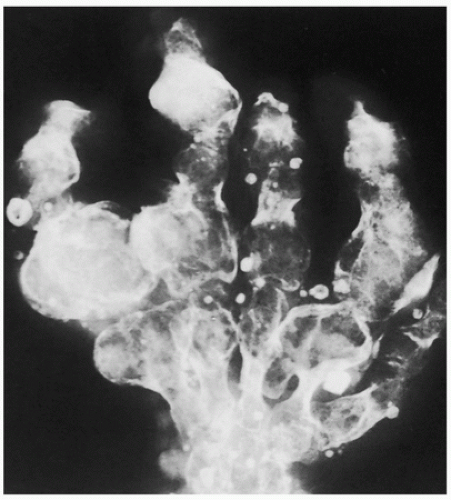 FIGURE 3.17 Radiography of Maffucci syndrome. Typical changes of this disorder consist of multiple enchondromas and softtissue hemangiomatosis, manifested by calcified phleboliths. |
▪ Periosteal osteoblastoma
Thin shell of newly formed periosteal bone usually covers the lesion.
Bone formation within the lesion.
Histopathology shows osteoid and immature bone trabeculae produced by osteoblasts.
Soft-Tissue Chondroma
Sites:
Hands and feet.
Clinical Findings:
Usually asymptomatic.
Imaging:
Radiography shows small (2 to 4 cm) well-defined softtissue masses with chondroid type of calcifications.
Pathology:
Gross (Macroscopy):
Well-circumscribed cartilaginous nodule.
Histopathology:
Lesion composed of lobules of hyaline cartilage covered by fibrous tissue (Fig. 3.24).
Sometimes partially myxoid, moderately cellular tissue with hyperchromatic nuclei.
May contain focal areas of fibrosis, hemorrhage, necrosis, calcifications, and granuloma formation.
 FIGURE 3.18 Radiography of Maffucci syndrome. Dorsovolar radiograph of the right hand of a 26-year-old woman shows multiple enchondromas affecting carpal bones, metacarpals, and phalanges. One of the lesions underwent malignant transformation to chondrosarcoma (arrows). Note numerous phleboliths within soft-tissue hemangiomas. |
Differential Diagnosis:
▪ Myositis ossificans
Imaging modalities and histopathology show lack of cartilage formation and classic zonal phenomenon (outer layer of mature bone formation and inner layer composed of reactive proliferation of spindle cells).
▪ Synovial sarcoma
Lower extremities more commonly affected.
May invade the adjacent bone.
Periosteal reaction may be observed.
MRI shows characteristic “triple-signal- intensity” pattern.
Histopathology shows biphasic appearance with gland-like spaces and spindle cell sarcomatous areas; positivity for epithelial membrane antigen (EMA) and for bcl2 and CD99, but negative for S-100 protein.
▪ Soft-tissue chondrosarcoma
Larger lesion.
Histopathology shows undifferentiated mesenchymal cells with only rare islands of well-differentiated cartilage; frequent myxoid changes; and permeation and entrapment of bone trabeculae.
 FIGURE 3.19 Radiography of periosteal chondroma. (A) Radiolucent lesion erodes the external surface of the cortex of proximal humerus (arrow) in this 24-year-old man. (B) Well-defined, saucer-like erosion of the cortex of the proximal phalanx is characteristic for this tumor. (C) Metaphyseal lesion erodes the cortex of the fifth metacarpal and evokes the buttress of periosteal reaction (arrow). |
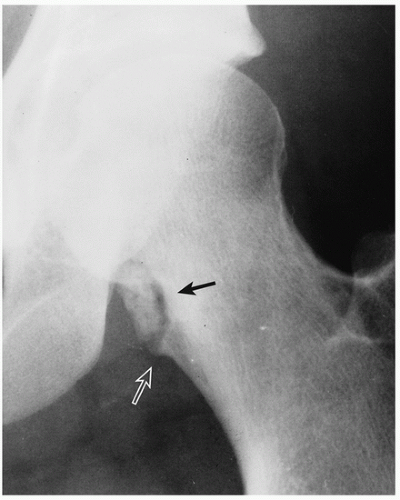 FIGURE 3.20 Radiography of periosteal chondroma. A cartilaginous lesion is eroding the medial cortex of the neck of the femur (arrow) evoking a buttress of periosteal reaction (open arrow). |
 FIGURE 3.21 Radiography and computed tomography of periosteal chondroma. (A) Lateral radiograph of the distal femur shows a bony excrescence arising from the posterior cortex, resembling an osteochondroma. (B) Conventional tomography demonstrates calcifications at the base of the lesion and lack of communication of the medullary cavities of the lesion and a host bone, as invariably is seen in osteochondroma. |
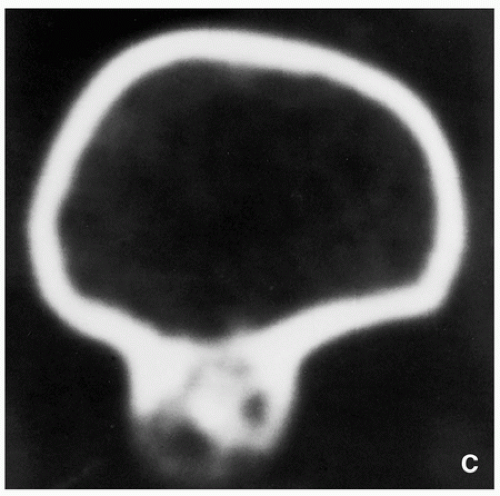 FIGURE 3.21 (Continued). (C) Computed tomography section demonstrates that the lesion is separated from the host bone by femoral cortex. |
 FIGURE 3.22 Radiography and magnetic resonance imaging of periosteal chondroma. (A) Radiography shows a large lesion that blends imperceptibly with the medial cortex of the fibula, extending into the medullary portion of the bone. (B) Coronal proton density and (C) sagittal T2-weighted MR images show the lesion’s extension into the medullary cavity. |
Synovial (Osteo) Chondromatosis
Definition:
Benign metaplastic nodular cartilaginous proliferation arising in the synovial membrane of joints, bursae, or tendon sheaths.
Epidemiology:
Uncommon condition.
Mostly seen in adults.
Male-to-female ratio of 2:1.
Sites of Involvement:
Most of the time only one joint is involved.
Most common involvement of the knee followed by the hip, elbow, wrist, ankle, and shoulder joint.
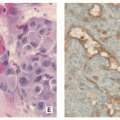
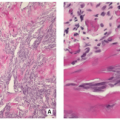
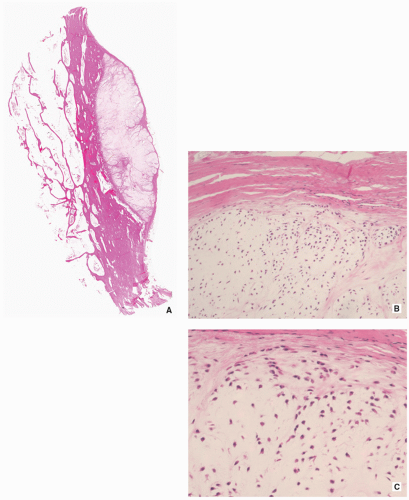 FIGURE 3.23 Histopathology of periosteal chondroma. (A) At the interface with the adjacent cortex, the cartilaginous tumor (right) erodes the bone (H&E, whole-mount section). (B) The higher magnification shows the tumor tissue more cellular than that of enchondroma, with some cells appearing atypical (H&E, original magnification ×100). (C) High magnification shows hyaline cartilage with rather dense cell population and slight cell enlargement, typical for this type of cartilage tumor (H&E, original magnification ×200). |
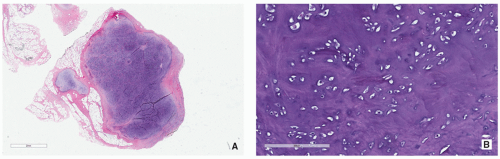 FIGURE 3.24 Histopathology of soft-tissue chondroma. (A) Lesion is composed of well-circumscribed hyaline cartilage covered by fibrous tissue (H&E, original magnification ×10). (B) Higher-magnification photomicrograph shows moderately cellular hyaline cartilage. Note benign chondrocytes with hyperchromatic nuclei (H&E, original magnification ×200). |
Clinical Findings:
Nonspecific symptoms with recurrent pain, swelling, joint effusion, and stiffness of joint.
Sometimes lesion may present as painless soft-tissue mass adjacent to a joint.
Imaging:
Radiographic findings depend upon the degree of calcification within the cartilaginous bodies, ranging from joint effusion only to visualization of many radiopaque joint bodies (Figs. 3.25 and 3.26). The bodies are small and uniform in size.

FIGURE 3.25 Radiography of synovial (osteo)chondromatosis. (A) Anteroposterior and (B) lateral radiographs of the elbow of a 27-year-old man show multiple osteochondral bodies within the joint, regularly shaped and uniform in size.
CT and MRI demonstrate intra-articular loose bodies (even noncalcified), bone erosion, and (rare) extracapsular extension of the lesion (Figs. 3.27, 3.28 and 3.29).
Pathology:
Gross (Macroscopy):
Multiple blue/white ovoid bodies or nodules within synovial tissue (Fig. 3.30).
Nodules may measure from a millimeters to several centimeters.
 FIGURE 3.26 Radiography of synovial (osteo)chondromatosis. (A) Anteroposterior and (B) frog-lateral radiographs of the right hip of a 59-year-old woman demonstrate numerous uniform in size intra-articular osteochondral bodies. |
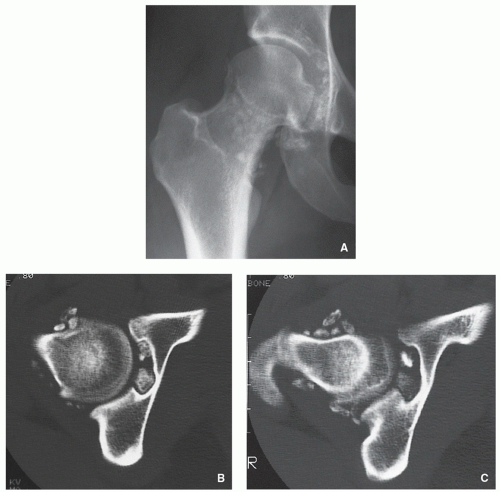 FIGURE 3.27 Radiography and computed tomography of synovial (osteo)chondromatosis. (A) Anteroposterior radiograph of the right hip of a 27-year-old woman shows multiple osteochondral bodies around the femoral head and neck. (B,C) Two axial CT sections, one through the femoral head and another through the femoral neck, demonstrate unquestionably the intra-articular location of multiple osteochondral bodies. |
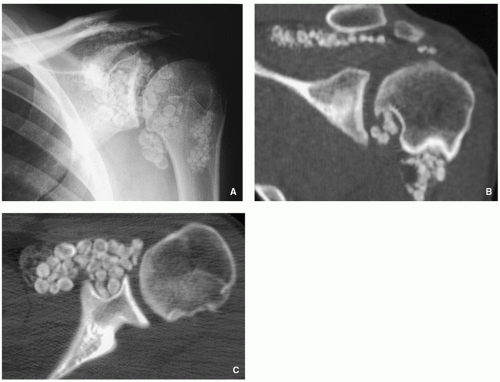 FIGURE 3.28 Radiography and computed tomography of synovial (osteo)chondromatosis. (A) Anteroposterior radiograph of the left shoulder of a 36-year-old man shows multiple osteochondral bodies around the glenohumeral joint. (B) Coronal CT section effectively shows location of the uniform in size calcified bodies in the glenohumeral joint and subacromial bursa. (C) Axial CT section confirms the intra-articular location of osteochondral bodies. |
Histopathology:
Variably cellular hyaline cartilage nodules covered by a fibrous tissue with synovial lining (Figs. 3.31 and 3.32A).
Chondrocytes may form clusters with plump nuclei, and some of them may show moderate nuclear enlargement and binucleated cells (Fig. 3.32B).
Uncommon mitotic figures.
Ossifications and fatty marrow in intertrabecular spaces may be seen.
Genetics:
Most cases show near-diploid or pseudodiploid karyotypes with some cases showing only simple numerical changes (-X, -Y, and +5, respectively).
Some cases may display rearrangement of the bands 1p13-p22.
Prognostic Factors/Complications:
Self-limiting process with potential local recurrence.
Bone erosion has been described.
Rare cases of chondrosarcoma arising in synovial chondromatosis were described.
Differential Diagnosis:
▪ Secondary osteochondromatosis (complication of osteoarthritis)
The osteochondral bodies are larger and not uniform in size.
Affected joint shows degenerative changes (osteoarthritis).
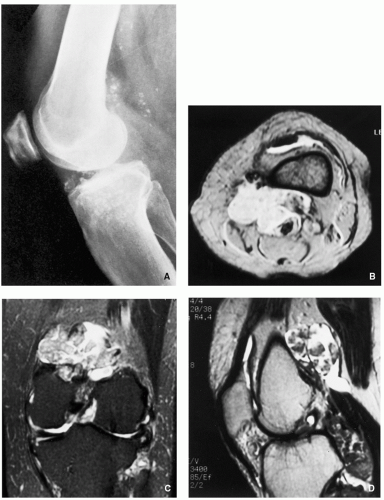 FIGURE 3.29 Radiography and magnetic resonance imaging of synovial (osteo)chondromatosis. (A) Lateral radiograph of the left knee of a 50-year-old man shows multiple osteochondral bodies in and around the joint. (B) Axial T2*-weighted (MPGR) MR image demonstrates high signal intensity joint effusion and multiple bodies of intermediate signal intensity, primarily located in a large popliteal cyst. (C) Coronal T2-weighted fat-suppressed and (D) sagittal fast spin echo MR images show to better advantage the distribution of numerous osteochondral bodies. |
 FIGURE 3.30 Gross specimen of synovial (osteo)chondromatosis. Multiple blue/white ovoid nodules of cartilage are scattered within the synovial tissue. |
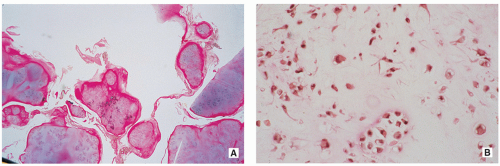 FIGURE 3.31 Histopathology of synovial (osteo)chondromatosis. (A) Photomicrograph of the synovium removed from the knee of a patient with primary synovial (osteo)chondromatosis shows nodules of irregular cellular cartilage covered by a thin layer of synovium (H&E, original magnification ×6). (B) High-power photomicrograph shows cells arranged in clusters with dark nuclei (H&E, original magnification ×100). |
 FIGURE 3.32 Histopathology of synovial (osteo)chondromatosis. (A) Variable cartilaginous nodules are covered by synovial tissue (H&E, original magnification ×100). (B) On higher magnification, note the clusters of chondrocytes with plump nuclei. Some of the cells show binucleation (H&E, original magnification ×200). |
Osteochondroma (Osteocartilaginous Exostosis)
Definition:
Cartilage-capped osseous projection (either sessile or pedunculated) arising on the external surface of a bone exhibiting an uninterrupted merging of the cortex of the host bone with the cortex of the lesion and communication of the medullary portions of the lesion and adjacent bone.
Epidemiology:
Most common benign bone lesion (20% to 50% of all benign bone tumors).
May be solitary or multiple, the latter occurring in the setting of hereditary multiple exostoses.
Solitary lesions account for 80% of cases.
Most common in the second decade of life.
Male-to-female ratio of 1.5-2:1.
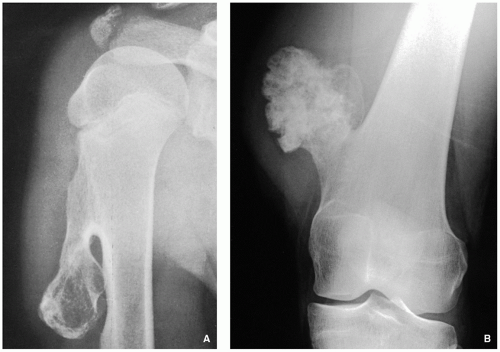 FIGURE 3.33 Radiography of pedunculated osteochondroma. (A) The typical pedunculated variant of this lesion is seen arising near the proximal growth plate of the right humerus of a 13-year-old boy. Note continuity of the cortex of the lesion with the cortex of a host bone and communication of their respective medullary cavities. (B) Pedunculated osteochondroma arising from the medial cortex of the distal left femur of a 22-year-old woman exhibits calcifications in the chondro-osseous zone of the stalk. |
Sites:
Most common sites: metaphyseal region of the distal femur, proximal humerus, and proximal tibia and fibula.
Clinical Findings:
Most common presentation is that of a hard mass of longstanding duration.
Majority of the lesions are asymptomatic and found incidentally.
Symptoms are often related to the size and location of the lesion, pressure on the nerve or blood vessels, pathologic fracture, or bursitis exostotica.
Imaging:
Radiography shows bulbous, cauliflower-like lesions (Fig. 3.33).
The characteristic feature is continuation of the cortex of the lesion with that of a host bone and communication of the respected medullary portions (Figs. 3.34, 3.35 and 3.36).

FIGURE 3.34 Radiography of sessile osteochondroma. (A) Broad-based lesion is seen arising from the medial cortex of the proximal diaphysis of the right humerus of a 14-year-old boy. Dense calcifications are present at the chondro-osseous junction of the lesion. (B) Lateral radiograph of the ankle of a 26-year-old woman shows a sessile osteochondroma arising from the posterior aspect of distal tibia.

FIGURE 3.35 Radiography of sessile osteochondroma. (A) Anteroposterior and (B) lateral radiographs of the right knee of a 57-yearold woman show a sessile lesion arising from the posteromedial aspect of the distal femur, showing continuity of the cortex and medullary cavities of the lesion and host bone, and displaying no visible calcifications.

FIGURE 3.36 Radiography of sessile osteochondroma. Anteroposterior radiograph shows a large sessile lesion arising from the lateral aspect of the proximal humeral diaphysis of an 11-yearold girl. Note that the cortex of the lesion and the host bone are in continuity, and the medullary portions are communicating.
Calcifications in the chondro-osseous junction of the lesion (see Figs. 3.33B and 3.34A).
Excessive cartilage-type flocculent calcifications, particularly dispersed calcifications into the cartilaginous cap, should raise the suspicion of malignant transformation (see Fig. 3.46 and Table 3.1).
TABLE 3.1 Clinical and Imaging Features Suggesting Malignant Transformation of Osteochondroma
Clinical Features
Radiologic Findings
Imaging Modality
Pain (in the absence of fracture, bursitis, or pressure on nearby nerves)
Enlargement of the lesion
Conventional radiography (comparison with earlier radiographs)
Growth spurt (after skeletal maturity)
Development of a bulky cartilaginous cap usually more than 2-3 cm thick
CT, MRI
Dispersed calcifications in the cartilaginous cap
Development of a soft-tissue mass with or without calcifications
Radiography, CT, MRI
Increased uptake of isotope after closure of growth place (not always reliable)
Scintigraphy
From Greenspan A, Beltran J. Orthopedic Imaging. 6th ed. Wolters Kluwer: Philadelphia 2015:745, Table 18.1.
CT and MRI typically show unequivocally the lack of cortical interruption and the continuity of cancellous portions of the lesion and the host bone (Figs. 3.37, 3.38 and 3.39). These modalities also demonstrate the thickness of the cartilaginous cap.
Pathology:
Gross (Macroscopy):
May be sessile (Fig. 3.40) or pedunculated.
The cortex and medullary cavity of the host bone extend into the lesion.
The cartilage cap is usually thin.
A thick cap (greater than 2 cm) may be indicative of malignant transformation.
Histopathology:
The lesion has three layers—perichondrium (fibrous layer covering cartilage), cartilage, and bone (Figs. 3.41 and 3.42).
The outer layer is a fibrous perichondrium that is continuous with the periosteum of the underlying bone.
Underneath there is a cartilage cap that is usually less than 2 cm thick (thickness decreases with age).
Within the cartilage cap, the superficial chondrocytes are clustered, whereas the ones close to bone resemble growth plate.
Loss of the architecture of cartilage, wide fibrous bands, myxoid change, increased chondrocyte cellularity, mitotic activity, significant chondrocyte atypia, and necrosis are all features that may indicate secondary malignant transformation.
Genetics:
Chromosomal aberrations involving EXT1 gene 8q22-24.1 and EXT2 11p11-p12 defect.
 FIGURE 3.37 Radiography and computed tomography of osteochondroma. (A) Lateral radiograph of the knee shows a calcified lesion at the posterior aspect of the proximal tibia (arrows). The exact nature of the lesion cannot be ascertained. (B) CT section clearly establishes continuity of the cortex, which extends without interruption from osteochondroma into the tibia. Note also that the medullary portions of the lesion and the tibia communicate. (C) In another patient, a 26-year-old woman, a radiograph of the right hip shows a heavy calcified lesion arising from the intertrochanteric area of the femur. (D) CT section demonstrates a cauliflower-like mass exhibiting thin cartilaginous cap. |
 FIGURE 3.38 Radiography, computed tomography, and magnetic resonance imaging of sessile osteochondroma. (A) Anteroposterior radiograph of the left hemipelvis of a 29-yearold man shows a large cartilaginous lesion arising from the ilium. (B) Axial CT shows better the relationship between the lesion and the host bone. (C) Axial T2-weighted MR image demonstrates high signal intensity of the cartilaginous cap. (D) Coronal T1-weighted fatsuppressed MR image obtained after intravenous administration of gadolinium shows peripheral enhancement of the fibrovascular layer, which covers nonenhancing cartilaginous cap of the lesion (arrows). |
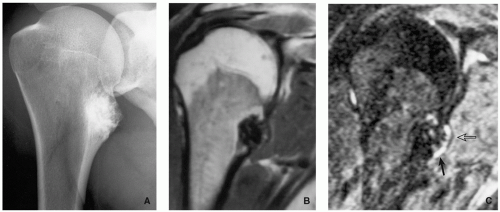 FIGURE 3.39 Radiography and magnetic resonance imaging of osteochondroma. (A) Radiograph of the right shoulder shows a sessile lesion at the medial aspect of the proximal humerus. (B) Coronal T1-weighted MR image reveals that the lesion exhibits low signal intensity due to heavy mineralization. (C) T2-weighted MRI shows a thin cartilaginous cap covering the lesion that exhibits high signal intensity (arrow), covered by linear strip of low signal intensity, representing perichondrium (open arrow). |
Complications:
Fracture of the lesion.
Pressure/erosion and fracture of the adjacent bone (ulna, fibula) (Figs. 3.43 and 3.44).
Bursitis (bursa exostotica) (Fig. 3.45).
Pressure on nerves and blood vessels.
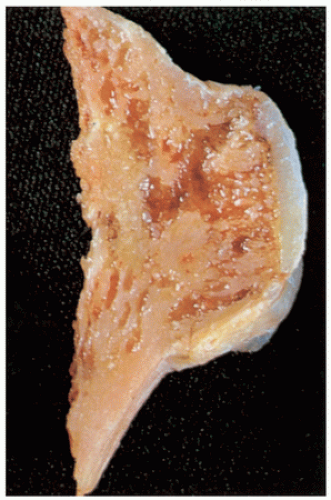
FIGURE 3.40 Gross specimen of sessile osteochondroma. Note continuity of the cortex and medullary cavities, and thin cartilaginous cap.
Malignant transformation to chondrosarcoma (less than 1% in solitary lesions) (Fig. 3.46).
Prognosis:
Excision is usually curative.
Recurrence is seen with incomplete removal.
Differential Diagnosis:
▪ Periosteal chondroma
Lesion separated from the host bone but may erode the cortex.
Large lesion may mimic osteochondroma but lack cortical and medullary continuity.
Value of attenuation coefficient of the lesion as determined by CT (Hounsfield values) is helpful in differential diagnosis: base of osteochondroma has higher values than does that of periosteal chondroma.
▪ Trevor-Fairbanks disease (dysplasia epiphysealis hemimelica, intra-articular osteochondroma)
Asymmetric cartilaginous overgrowth of one or more epiphyses.
Talus, distal femur, and distal tibia most commonly affected.
Histopathologically almost identical with osteochondroma.
▪ BPOP (Nora lesion, bizarre parosteal osteochondromatous proliferation)
Usually affects the metacarpals and phalanges of the hand.
Mushroom-like-shaped osseous or cartilaginous mass attached to the cortex.
Lack of communication with medullary cavity of the host bone.
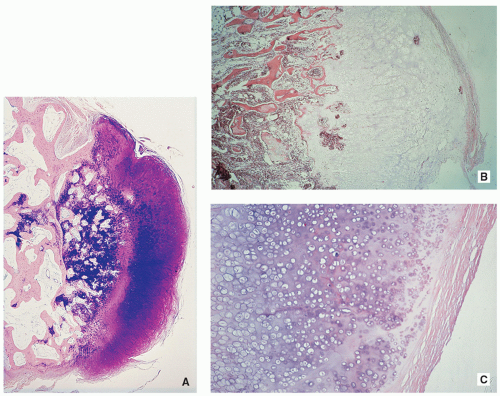 FIGURE 3.41 Histopathology of sessile osteochondroma. (A) The tumor consists of the hyaline cartilaginous cap with strong metachromasia of the matrix. A broad zone of endochondral ossification borders the cancellous bone containing the remnants of cartilaginous matrix (center) (Giemsa, original magnification ×6). (B) At higher magnification, foci of calcifications are seen at the chondroosseous junction. These areas correspond to a zone of provisional calcification in the growth plate. Beneath the cap, there is evidence of transformation of the cartilage into bone by process of endochondral ossification (H&E, original magnification ×30). (C) Periphery of the lesion consists of a hyaline cartilaginous cap, which is covered by a thin fibrous membrane (perichondrium) (H&E, original magnification ×60). |
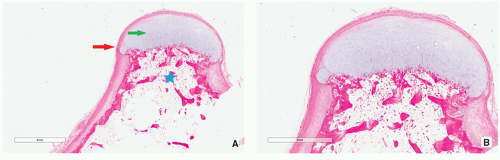 FIGURE 3.42 Histopathology of pedunculated osteochondroma. (A) The lesion consists of three layers: outer fibrous layer of perichondrium (red arrow), cartilaginous cap (green arrow), and osseous stalk (star) (H&E, original magnification ×5). (B) Higher magnification shows continuation of the perichondrium with the periosteum covering the stalk of the lesion (H&E, original magnification ×10). |
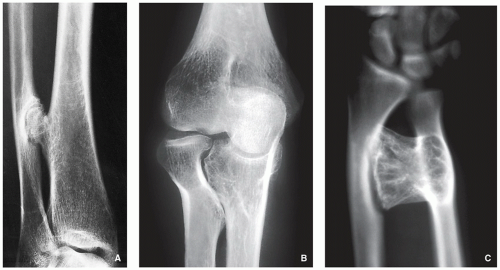 FIGURE 3.43 Complications of osteochondroma: pressure erosion of the adjacent bone. (A) Osteochondroma arising from the posterolateral aspect of the right distal tibia of a 24-year-old man has eroded the adjacent fibula. (B) In another patient, continued growth of the sessile osteochondroma of the proximal ulna resulted in pressure erosion of the head and neck of the radius. (C) Pedunculated lesion of the distal ulna has eroded medial aspect of the shaft of the radius. |
 FIGURE 3.44 Complications of osteochondroma: fracture of the adjacent bone. The continued growth of a sessile osteochondroma of the distal tibial metaphysis of a 9-year-old boy has caused a fracture of the adjacent fibula. |
▪ Juxtacortical (parosteal) osteoma
Homogenously dense, sclerotic, ivory-like mass.
No communication with the medullary portion of the host bone.
Histopathology shows compact, dense, mature lamellar bone, or woven bone formation with transformation to lamellar bone, and osteocyte lacunae.
Multiple Hereditary Osteochondromata (Diaphyseal Aclasis)
Autosomal dominant genetic disorder with incomplete penetrance in females.
Male predominance 2:1.
Most commonly affected sites are the knees, ankles, and shoulders.
Imaging features similar to single osteochondromas, but lesions more commonly of sessile type (Figs. 3.47, 3.48, 3.49, 3.50, 3.51 and 3.52).
Growth disturbance (dysplastic changes, retardation of longitudinal bone growth) (Figs. 3.48, 3.49, 3.50, and 3.53).
Histopathologic features identical to those of solitary lesions.
Genetic defect has recently been identified, a novel mutation in genes EXT1 that maps to chromosome 8q24.1, EXT2 that maps to chromosome 11p11-p12, and EXT3 that maps to the short arm of chromosome 19.
 FIGURE 3.45 Complications of osteochondroma: bursa exostotica. (A) A 25-year-old man with a known solitary osteochondroma of the distal right femur presented with gradually increased pain. Malignancy was suspected, and arteriography was performed. The capillary phase of the arteriogram reveals a huge bursa exostotica, one of the complications of osteochondroma. (B) Coronal T1-weighted MR image of a 12-year-old girl who presented with pain in the popliteal fossa demonstrates a large osteochondroma arising from the posterolateral aspect of the distal femur (arrow). (C) Axial T2-weighted MRI shows a bursa exostotica distended with high-intensity fluid (arrows). |
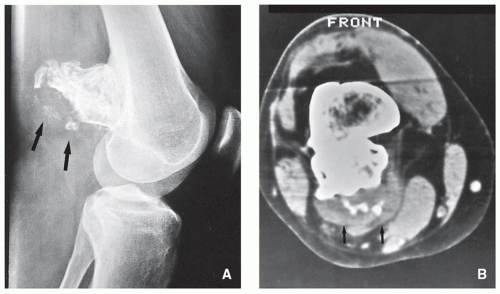 FIGURE 3.46 Complications of osteochondroma: malignant transformation. (A) Lateral radiograph of the knee of a 28-year-old man, who presented with pain in the popliteal region and increase in size of the mass he had been aware of for 15 years, shows a sessile osteochondroma arising from the posterior cortex of the distal femur. Note that calcifications not only are present at the chondro-osseous junction of the lesion but also are dispersed in the cartilaginous cap (arrows). (B) CT section confirms the increased thickness of the cartilaginous cap and dispersed calcifications within it (arrows), features of malignant transformation to chondrosarcoma, which was confirmed on histopathologic examination. |
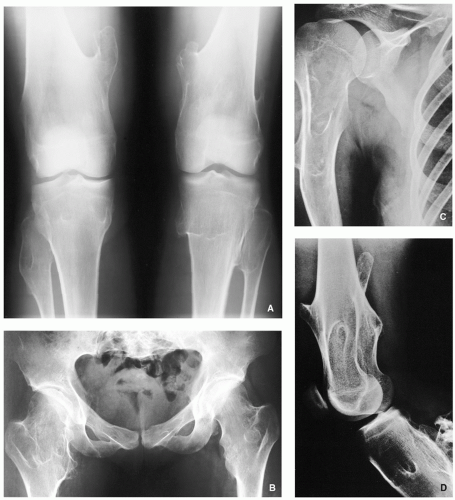 FIGURE 3.47 Radiography of multiple osteocartilaginous exostoses. (A) Anteroposterior radiograph of both knees of a 17-yearold boy shows numerous sessile and pedunculated osteochondromas. (B) Anteroposterior radiograph of the pelvis demonstrates numerous sessile osteochondromas affecting proximal femora. (C) Anteroposterior radiograph of the right shoulder of a 22-year-old man shows multiple sessile lesions involving the proximal humerus and scapula. (D) Lateral radiograph of the knee of the same patient shows involvement of the distal femur and proximal tibia. |
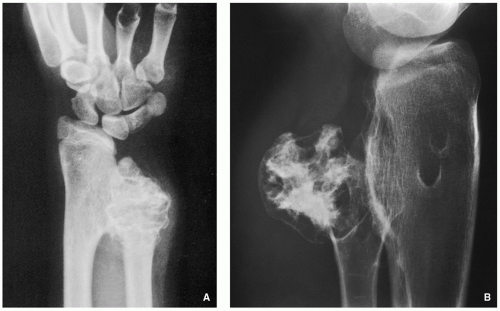 FIGURE 3.48 Radiography of multiple osteocartilaginous exostoses. (A) Radiograph of the distal forearm of an 8-year-old boy shows growth disturbance in the distal radius and ulna. (B) In another patient, a 21-year-old woman, observe growth disturbance of the proximal fibula. |
Chondroblastoma
Definition:
Benign, cartilage-producing neoplasm usually arising in the epiphyses of long bones of skeletally immature patients.
Epidemiology:
Accounts for less than 1% of primary bone tumors.
Most common between 10 and 25 years of age.
Male predominance.
Patients with skull and temporal bone involvement tend to present at an older age (40 to 50 years).
Sites of Involvement:
Mostly involve epiphyses of the distal and proximal femur, followed by the proximal tibia and proximal humerus.
Patients with tumors arising in the flat bones, vertebrae, and short tubular bones tend to be older and skeletally mature, although rare cases have been reported in children.
Clinical Findings:
Majority of patients complain of localized pain, often mild, but sometimes of many years’ duration.
Soft-tissue swelling, joint stiffness and limitation, and limp are reported less commonly.
Minority of patients may develop joint effusion, especially around the knee.
Imaging:
Typically radiolucent, centrally or eccentrically located, relatively small lesion (3 to 6 cm), occupying less than one-half of the epiphysis (Fig. 3.54).
Matrix calcifications are only visible in about one-third of patients.
Periosteal reaction remote from the tumor (see Figs. 3.56A and 3.57A).
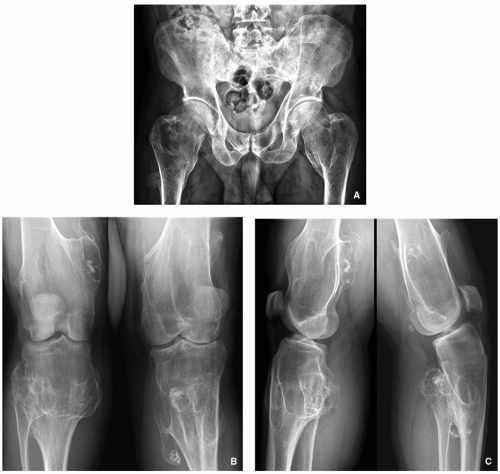 FIGURE 3.49 Radiography of multiple osteocartilaginous exostoses. (A) Anteroposterior radiograph of the pelvis of a 45-year-old man shows multiple lesions of the proximal femora. Note the broadening of the femoral necks. (B) Anteroposterior and (C) lateral radiographs of both knees of the same patient show classic appearance of this disorder: numerous sessile and pedunculated osteochondromas are seen arising from the distal femora and proximal tibiae and fibulae. Note also the growth disturbance due to defective metaphyseal remodeling commonly seen in this condition. |
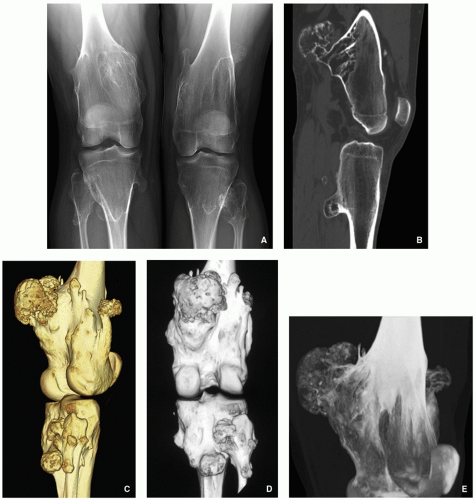 FIGURE 3.50 Radiography and computed tomography of multiple osteocartilaginous exostoses. (A) Anteroposterior radiograph of both knees of a 20-year-old man shows multiple osteochondromas arising from the distal femora and proximal tibiae and fibulae, associated with growth disturbance reflected by Erlenmeyer flask deformities. (B) Sagittal reformatted CT image shows osteochondromas arising from the posterior aspect of the distal femur and proximal tibia. Three-dimensional CT images with surface-rendering algorithm viewed from the lateral (C) and posterior (D) aspects of the knee show spatial distribution of numerous osteochondromas. (E) 3D CT image of the distal femur in maximum intensity projection (MIP) shows interior architecture of one of the sessile lesions. |
 FIGURE 3.51 Computed tomography of multiple osteocartilaginous exostoses. Three-dimensional angio-CT image of the pelvis with surface-rendering algorithm of a 57-yearold woman shows multiple osteochondromas arising from the iliac wings, pubic bones, and proximal femora. The iliac and femoral arteries were not affected by the exostoses. |
Pathology:
Gross (Macroscopy):
Gritty and grayish white mass with areas of hemorrhage.
Histopathology:
Densely cellular tissue composed of an admixture of mononuclear chondroblasts and multinucleated osteoclast-type giant cells (Fig. 3.59A).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree