Outline
Topic 9, Figure 319
- 1.
Fig. 319 . Topic: Information on the 3D Volume Set Screen Is Abundant.

Fig. 319
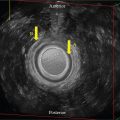
A good 3D volume set will provide much information all on one screen. This is a transperineal 3D volume set with a rendered view of a 75-year-old patient who has trouble voiding and a history of a urethral sling placement for urinary incontinence. A second rendered image is shown (screen right).
The acquisition A plane is a midsagittal cut of the urethra, which is compressed anteriorly at the mid-distal segment by the echogenic sling (yellow arrow), causing a widened proximal urethra (red arrow), a very thin mid segment, and a short distal segment (white arrow). The B plane is posterior to the urethra and demonstrates a coronal cut of the sling at the center reference point (CRP) of the A plane. The C plane is an axial cut of the sling, seen posterior to the compressed urethra (green arrow). Remember to take advantage of the vertical and horizontal partial lines along the edges of the images, which would intersect at the CRP.
The green square icon seen along the side of the A and B images indicates the right side of the patient. The green diamond on image C indicates the anterior direction. The green line of reference is brought down to the CRP to provide the best rendered view of the mid-distal sling placement.
The screen bottom right image of the volume set is the rendered view of the urethra and the sling posterior to it. Notice the atypical appearance of the compressed urethra (green arrow) on the 3D rendered images. This compression results in the widened proximal urethra and the markedly enlarged bladder, partially seen as prolapsing inferior-posteriorly.
Case 151, Figures 320 and 321
- 2.
Fig. 320 is a transperineal 3D volume set of a 54-year-old patient with stress urinary incontinence, which had worsened since a mid-urethral sling placed at an outside institution was “resected.”

Fig. 320
The orthogonal planes of the 3D volume set as related to the urethra are relative to what the examiner uses as the original acquisition sweep plane. In this case, the volume sweep is made at a midline (ML) sagittal cut; therefore, the A plane image is a sagittal cut through the urethra.
As shown on Fig. 320 , the B plane is perpendicular to the A plane (light blue vertical line) at the CRP. It is coronal on the patient and posterior to the urethra. The C plane is coronal to the A plane, as seen at the red horizontal line. It is axial on the patient at the proximal urethra.
From Figs. 320 and 321 , assess the overall appearance of the urethra on the orthogonal planes as well as the 3D rendered urethral image.
- a.
Is the urethra irregular or smooth in contour? _____
- b.
Is there evidence of full, partial, or no residual hyperechoic mesh? _____
- c.
Remember, the top of the screen on a transperineal image is inferior, so the bottom of the screen is superior on the patient. The 3D rendered image (bottom right) is as if the viewer is looking from above into the green line of reference on A and B planes, which is “up” the urethra and superior on the patient (toward the proximal urethral level). Screen left of the rendered image (bottom right) is the patient’s right side. Is the residual mesh seen on the rendered image primarily to the left, at the central, or to the right of ML location(s)? _____

Fig. 321
- a.
- 3.
On Fig. 320 , note that the CRP is seen on all three planes at the residual mesh location (white arrow). Where the CRP is placed is the examiner’s decision, depending on the purpose of the specific volume planes. On the A plane, is the CRP seen posterior to the proximal, mid, or distal aspect of the urethra? _____
- 4.
Moving the CRP is the examiner’s role at the time of the exam depending on the desired visualization of a specific area of interest. It can also be moved at the 3D workstation post exam to move through the saved volume. Why is the mesh seen but the urethra not seen on the B plane?
- a.
It is not seen because the B cut is anterior to the urethra as seen on the A plane by the CRP location.
- b.
It is not seen because the B cut is to the right of the urethra as seen on the A plane by the CRP location.
- c.
It is not seen because the B cut is posterior to the urethra as seen on the A plane by the CRP location.
- d.
It is not seen because the B cut is to the left of the urethra as seen on the A plane by the CRP location.
- a.
- 5.
Does the mesh appear symmetric or asymmetric on the 3D rendered image? _____
Case 152, Figures 322–327
- 6.
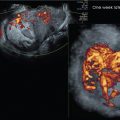
Figs. 322–327 are endovaginal (EV) images, using a 3–9 MHz transducer, of a 26-year-old who was diagnosed with a right-sided 4 × 4 cm tubo-ovarian abscess (TOA) from an ultrasound exam done at an outside institution 6 weeks ago. Her last menstrual period (LMP) was 8 days ago. Fig. 322 is a midsagittal uterine image. There is minimal posterior cul de sac (PCDS) free fluid (FF) present on today’s exam (blue arrow) compared with the last exam, at which time there was moderate FF noted. The left ovary appears within normal limits (WNL) ( Fig. 323 ). Answer the following questions. In what position is the uterus—anteverted (AV), retroverted (RV), anteflexed (AF), retroflexed (RF), or neutral?
- a.
AV
- b.
RV
- c.
AV, AF
- d.
Neutral
- e.
RV, RF

Fig. 322

Fig. 323
- a.
- 7.
In what phase of the cycle is the endometrium?
- a.
Early proliferative
- b.
Late proliferative
- c.
Mid-cycle
- d.
Early secretory
- e.
Late secretory
- a.
- 8.
Figs. 324 and 325 . Which of the following best describes the measured 3.51 × 2.28 × 2.45 cm component of the right ovary that measures smaller than the previously reported size of 4 × 4 cm?
- a.
Oval-shaped, thick-walled intraovarian lesion with hyperechoic central area
- b.
Thick-walled intraovarian lesion with heterogeneous hypoechoic central area
- c.
Round, thick-walled intraovarian lesion with anechoic central area
- d.
Oval-shaped, thin-walled intraovarian homogeneous hypoechoic central lesion

Fig. 324

Fig. 325
- a.
- 9.
Figs. 326 and 327 . No Doppler spectral waveform, including the resistive index (RI) of the area of concern, was obtained on the first exam. Which Color Power Doppler description below best characterizes the intraovarian lesion?
- a.
Diffusely vascular with high RI
- b.
Centrally vascular with low RI
- c.
Peripherally vascular with a low RI
- d.
Peripherally vascular with a high RI

Fig. 326

Fig. 327
- a.
Case 153, Figures 328–331
- 10.
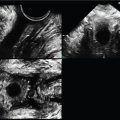
Figs. 328–331 demonstrate EV 2D and 3D volume set images, using a 5–9 MHz EV transducer, of the retroverted uterus on a 45-year-old female with a history of pelvic pain. The patient has a negative human chorionic gonadotropin (hCG). Her LMP was 19 days ago. In what position is the uterus? _____
- 11.
In what phase of the endometrial cycle is the sonographic appearance?
- a.
Post-menses
- b.
Proliferative
- c.
Mid-cycle
- d.
Secretory
- a.
- 12.
Fig. 328 demonstrates an oval anechoic structure labeled “A”. Fig. 329 is the 3D volume set with the acquisition sweep at midline sagittal and the CRP placed at the central endometrium. Now an additional anechoic structure labeled “B” measuring less than 1 mm in diameter is seen. Are the anechoic structures identified as “A” and “B” intraendometrial or at the endometrial/myometrial interface? _____

Fig. 328

Fig. 329
- 13.
Fig. 329 . The 3D rendered image has been removed. The “C” plane of the 3D volume set has been rotated counterclockwise (curved arrow) to be upright on the Z-axis. What additional finding (green arrows) is noted?
- a.
Peri-ovarian free fluid
- b.
Bilateral diffuse ovarian follicles
- c.
Tortuous peripheral vasculature
- d.
Normal uterine appearance
- a.
- 14.
How does the Color Power Doppler, as seen on Fig. 330 , support the negative hCG? _____

Fig. 330
- 15.
By moving the CRP on the C plane to structure A on Fig. 331 , all three planes visualize the larger lesion. Which of the following is the best sonographic diagnosis for these findings? _____
- a.
Endometrial cavity free fluid
- b.
Resorbing gestational sac
- c.
Endometrial cysts
- d.
Spiral artery
- e.
Adenomyosis
- f.
Intrauterine pregnancy (IUP)
- a.