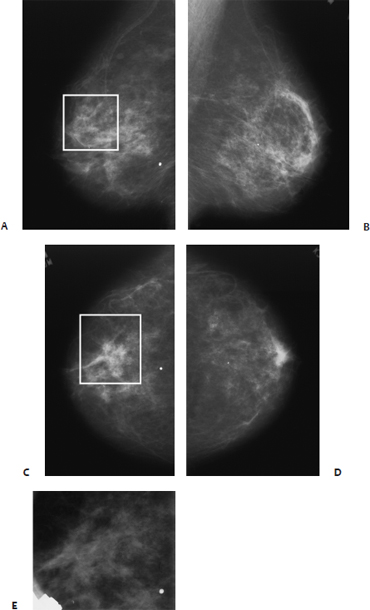
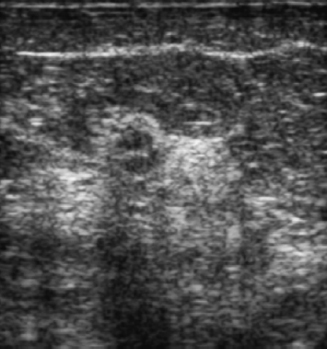
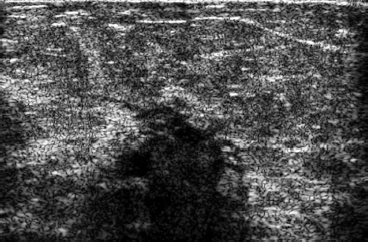
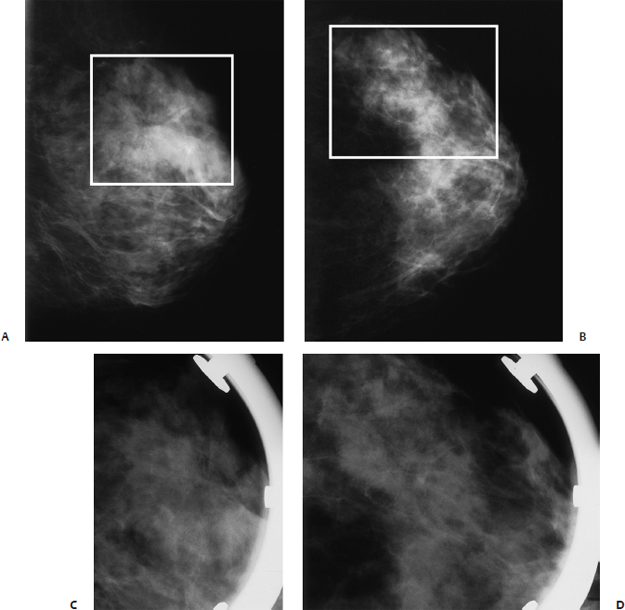
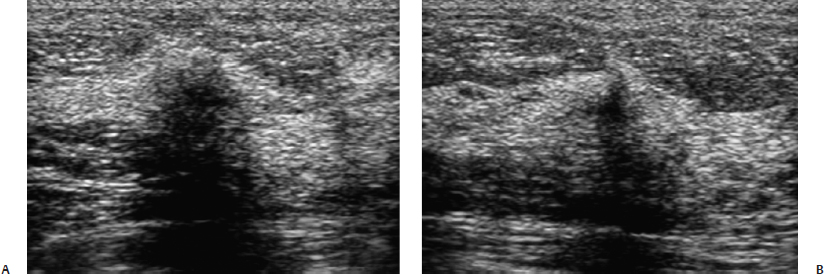
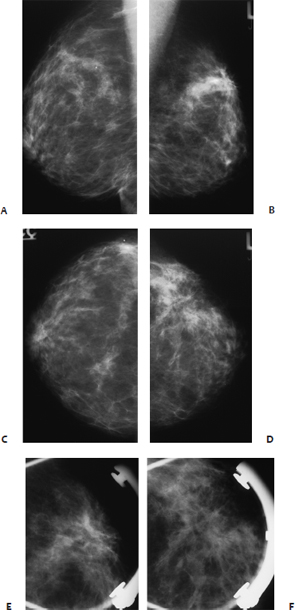
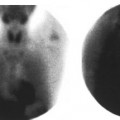
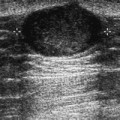
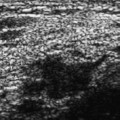
23 Central Architectural Distortion A 71-year-old woman presents for screening mammogram. • Architectural distortion (Fig. 23.1) • Normal exam Fig. 23.1 In the upper outer quadrant of the right breast, there is architectural distortion (square). Focal increased density was demonstrated only on the CC view. (A) Right MLO mammogram. (B) Left MLO mammogram. (C) Right CC mammogram. (D) Left CC mammogram. (E) Right CC spot compression mammogram. Low Frequency (Fig. 23.2) Frequency • 7 MHz Mass • Margin: ill defined • Echogenicity: hypoechoic • Retrotumoral acoustic appearance: posterior shadowing distal to mass • Shape: irregular Fig. 23.2 Right antiradial breast sonogram. With lower frequency, the mammographic architectural distortion is an irregular hypoechoic mass with posterior acoustic shadowing. Frequency • 10 MHz High-Frequency Findings This case illustrates that weaker penetration with higher frequency causes increased shadowing with benign masses as well as malignant ones. In this case, lower frequency is more useful than high frequency to identify the location of the mass. Fig. 23.3 Right antiradial breast sonogram. Higher-frequency examination produces extensive shadowing. The mass identified in Fig. 23.2 is hidden in the area of shadowing. • Sclerosing adenosis • BI-RADS assessment category 4, suspicious; biopsy should be considered. • Sclerosing adenosis is present in 3.1% of breasts. This lesion may present as a palpable mass and is occasionally associated with tenderness. • Mammographically, sclerosing adenosis produces architectural distortion with or without a focal mass and may simulate malignancy. • Sonographically, sclerosing adenosis is an irregular hypoechoic mass that cannot be differentiated from malignancy. Tabar L, Dean PB. Teaching Atlas of Mammography. 3rd ed. New York: Thieme; 2001:2–3, 197 Tavassoli FA. Pathology of the Breast. 2nd ed. Stamford Appleton & Lange; 1999 130–133 A 58-year-old woman presents for screening mammogram. • Normal exam • Architectural distortion (Fig. 23.4) Fig. 23.4 In the left upper outer quadrant, there is a spiculated density on the MLO view, which is less apparent on the CC view. Area of architectural distortion is surrounded by a square. (A) Left MLO mammogram. (B) Left CC mammogram. (C) Left MLO spot compression mammogram. (D) Left CC spot compression mammogram. Frequency • 7 MHz Mass (Fig. 23.5) • Margin: ill defined • Echogenicity: hypoechoic • Retrotumoral acoustic appearance severe shadowing, mass partially obscured • Shape: irregular Fig. 23.5 In the left upper outer quadrant, the mammographic architectural distortion corresponds to a lesion exhibiting severe shadowing. The lesion appears wide in the radial view (A) and narrow in the antiradial view (B). This extreme discrepancy in appearance is characteristic of either posttraumatic or radial scars. (A) Left radial breast sonogram. (B) Left antiradial breast sonogram. • Radial sclerosing lesion (radial scar) • BI-RADS assessment category 4, suspicious; biopsy should be considered. • Clinically, radial scars are generally not palpable. • Mammographically, radial scars commonly exhibit thin radiating lines without a central dense mass. The abnormality commonly changes appearance from one projection to another. • Sonographically, radial scars are similar in appearance to surgically produced scars. Radial scars exhibit a large hypoechoic or shadowing area in one view and a thin abnormality in the orthogonal view. The sonographic appearance should not prevent biopsy and excision of this lesion because about one third of radial scars are associated with ductal carcinoma in situ or tubular carcinoma. Evans AJ, Wilson ARM, Blamey RW, Robertson JFR, Ellis IO, Elston CW. Atlas of Breast Disease Management. Philadelphia: WB Saunders; 1998:94–97 Tabar L, Dean PB. Teaching Atlas of Mammography. 3rd ed. New York: Thieme; 2001:93–96, 102–106 A 63-year-old woman presents with a palpable lump in the left breast. Mass (Fig. 23.6) • Margin: spiculated • Shape: irregular • Density: equal density • Architectural distortion • Right breast normal • Left breast palpable mass in upper outer quadrant Fig. 23.6 In the upper outer left breast, there is a spiculated mass. (A) Right MLO mammogram. (B) Left MLO mammogram. (C) Right CC mammogram. (D) Left CC mammogram. (E) Left MLO spot compression mammogram. (F) Left CC spot compression mammogram. Frequency • 7 MHz Mass (Fig. 23.7) • Margin: ill defined • Echogenicity: hypoechoic • Retrotumoral acoustic appearance severe shadowing, mass partially obscured • Shape: irregular
Case 23.1: Sclerosing Adenosis
Case History
Mammogram
Physical Examination
Ultrasound
Pathology
Management
Pearls and Pitfalls
Suggested Reading
Case 23.2: Radial Scar
Case History
Physical Examination
Mammogram
Ultrasound
Pathology
Management
Pearls and Pitfalls
Suggested Reading
Case 23.3: Infiltrating Ductal
Case History
Mammogram
Physical Examination
Ultrasound
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


