Chapter 32 Cervical Zygapophysial Joint Intraarticular Injection, Lateral Approach
Note: Please see page ii for a list of anatomical terms/abbreviations used in this book.
Cervical zygapophysial joints (Z-joints) extend from C2-C3 to C7-T1. Injuries to these joints present as neck pain, and they are commonly the result of a whiplash injury or degenerative joint disease. The cervical axial pain can extend from the suboccipital region to the midscapular area, depending on the Z-joints involved. The most commonly involved joints are C2-C3 and C5-C6.1 Upper cervical joint injections (i.e., C2-C3 and C3-C4) should be considered for neck pain with associated headaches, whereas lower cervical joint injections (i.e., C5-C6 and C6-C7) should be considered for neck pain with associated shoulder pain.
In this chapter, the lateral approach to performing a cervical Z-joint intraarticular injection is described. Some may argue that the lateral approach is technically less demanding than the posterior approach: it can be performed with the use of a smaller-gauge needle (e.g., 25 or 26 gauge), and less soft tissue is traversed, thereby making it more comfortable for the patient.2 Regardless of the approach used, the total volume of anesthetic and steroid injected should be less than 1 mL3 to prevent the rupture of the joint capsule and leakage into adjacent structures.
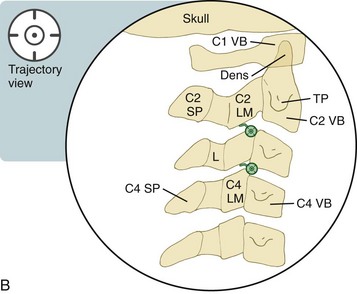
The higher cervical Z-joints are featured in this chapter, because the shoulders can obscure the fluoroscopic images. This approach can be more challenging in the lower segments. With the lateral approach, the trajectory view is the same as the lateral view. In addition to the lateral and anteroposterior views, a foraminal oblique view (see Chapter 3) can be used when there is difficulty visualizing the joint or to confirm needle placement in the correct cervical Z-joint. When performing cervical Z-joint injections, contrast flow into the space of “Okada” is a common phenomenon.4 The space of Okada is an extradural space dorsal to the ligamentum flavum. Contrast injection will flow initially into the Z-joint and then out the inferior recess of the joint and track medially into this retroligamentous space (see Figure 32–5).
 Trajectory View (
Trajectory View (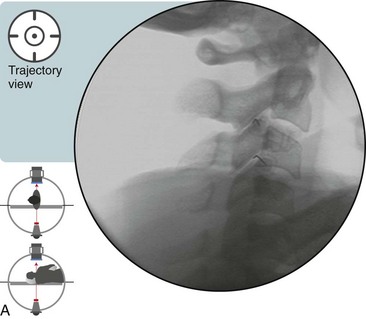
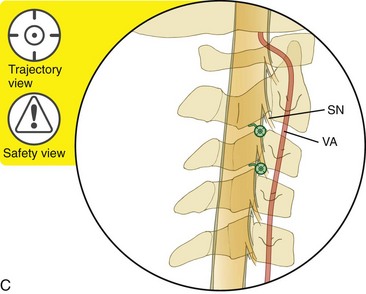
 Trajectory View Safety Considerations
Trajectory View Safety Considerations

 The Trajectory View (Lateral) is also a Multiplanar View
The Trajectory View (Lateral) is also a Multiplanar View
Place the patient in a lateral decubitus position with the symptomatic side up.
 Confirm the level using a lateral view (relative to the patient—zero degrees relative to the table if the patient lies perpendicular to it).
Confirm the level using a lateral view (relative to the patient—zero degrees relative to the table if the patient lies perpendicular to it).

 Because the patient is in a lateral decubitus position, the tilt will be used as discussed in Chapter 3.
Because the patient is in a lateral decubitus position, the tilt will be used as discussed in Chapter 3.
If needed, oblique the fluoroscope slightly so that the bilateral lateral masses line up.
Related posts:
 Atlantoaxial Joint Intraarticular Injection
Atlantoaxial Joint Intraarticular Injection
 Lumbar Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy, Posterior Approach
Lumbar Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy, Posterior Approach
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


