Chapter 31 Cervical Zygapophysial Joint Intraarticular Injection, Posterior Approach
Note: Please see page ii for a list of anatomical terms/abbreviations used in this book.
Cervical zygapophysial joints (Z-joints) extend from C2-C3 to C7-T1. Pain emanating from these joints commonly occurs as a result of a whiplash injury or from degenerative joint disease. The distribution of the axial cervical pain associated with these joints can extend from the suboccipital region to the midscapular region, depending on the Z-joints involved. Upper cervical Z-joint pain (i.e., C2-C3 and C3-C4) may present as neck pain with associated headaches, whereas lower cervical Z-joint pain (i.e., C5-C6 and C6-C7) may present as neck pain with associated shoulder or midscapular pain.1
In this chapter, the posterior approach for injecting the Z-joints is described. As compared with the lateral approach, the posterior approach allows for access to multiple joint levels on both sides of the spine, thereby negating the need to reposition the patient or C-arm when performing bilateral injections. This approach is often required for injecting the C7-T1 Z-joint, where the lateral approach may involve the risk of contacting the lung apex or the inferior neurovascular structures.2 With this approach, the trajectory view is an anteroposterior view with a caudad tilt (i.e., a pillar view), which also serves as the anteroposterior view with multiplanar imaging. Because the lateral view is used to assess depth, one need not step off of the inferior or superior articulation of the joint before penetrating the joint capsule, as is often recommended. Typically a 22- or 25-gauge needle is used to inject a maximum volume of 1 mL of a steroid and anesthetic mixture into each joint.
 Trajectory View (Figure 31–1)
Trajectory View (Figure 31–1)
 Confirm the level (with the anteroposterior view).
Confirm the level (with the anteroposterior view).
 Tilt the fluoroscope’s image intensifier caudally.
Tilt the fluoroscope’s image intensifier caudally.


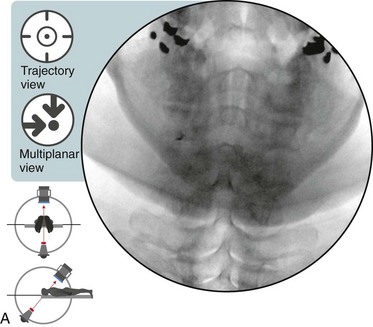
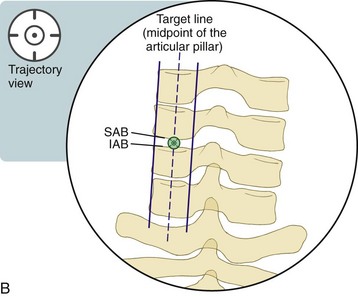
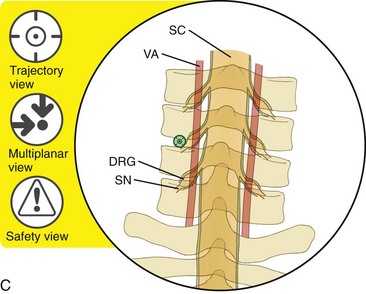
Figure 31–1 A,
Related posts:
 Atlantoaxial Joint Intraarticular Injection
Atlantoaxial Joint Intraarticular Injection
 Cervical Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy and Nerve Injection, Posterior Approach
Cervical Zygapophysial Joint Nerve (Medial Branch) Radiofrequency Neurotomy and Nerve Injection, Posterior Approach
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


