13.3 Injuries
13.3.1 Rib Contusions and Fractures
A direct trauma to the chest during sports participation may result in an injury to the ribs. The consequence may range from bruising or a rib contusion to a (un)displaced rib fracture. A rib fracture is a common sports injury in contact sports and is regularly caused by a fast and intense blow directly to the chest. Elbows and other body parts may cause a hard-enough strike, as may sports attributes as bats, sticks, or projectiles. Traumatic fractures of the first and second ribs suggest a very significant transfer of energy with the trauma and are associated with secondary injury to underlying neurovascular structures.
Following the direct trauma of motion that lead to the fracture, athletes will notice a sharp pain in the affected region. This pain can be aggravated by deep breathing, coughing, sneezing, or squeezing. Breathing symptoms may lead to quick, shallow breaths to avoid complaints. Examination reveals local tenderness over one or more ribs and with compression of the thorax. The area surrounding the injury may be bruised. Respiratory examination can be used to exclude pneumothorax.
13.3.2 Rib Stress Fracture
Most reports of stress fractures of the ribs in athletes concern the first rib. First-rib stress fractures are most often seen in overhead athletes. Baseball, basketball, or tennis players and weightlifters are typically at risk (Aitken and Lincoln 1939; Brooke 1959; Gregory et al. 2002). Repetitive contraction of the anterior scalenus muscle causes bending stress on the subclavian sulcus, which is the most common area of first-rib stress fractures to occur (Gupta et al. 1997). Repetitive traction on the arm with a contracted scalenus muscle may have the same etiological effect; training mistakes may also contribute to the emergence of stress fractures (Bailey 1985; Brooke 1959; Lankenner and Micheli 1985).
Athletes with a stress fracture of the first rib will feel pain around the shoulder, the top of the scapula, or front of the neck, with possible radiation to the sternum and pectoral region. The onset is most often insidious, although acute onset also has been reported in cases (Gregory et al. 2002; Mamanee et al. 1999). Examination reveals tenderness medial to the superior angle of the scapula, at the root of the neck, at the supraclavicular triangle, or deep in the axilla (Bailey 1985; Gregory et al. 2002; Gurtler et al. 1985; Mintz et al. 1990). Shoulder movements may be restricted and painful.
Rib stress fractures to other ribs are less common and most often seen in high-level rowers or novice golf players (Bojanic and Desnica 1998; Christiansen and Kanstrup 1997; Holden and Jackson 1985; Lord et al. 1996). Among elite rowers incidences of 8.1–16.1 % were reported, while amateur rowers have a lower reported risk (McDonnell et al. 2011). In novice golf players, a poor technique or sudden increase in training load is thought to produce stress fractures (Gregory et al. 2002).
The injury mechanism of rib stress fractures in rowers is multifactorial, with intrinsic and extrinsic risk factors contributing to the emergence. A recent review suggests that the posterior-directed resultant forces from the combined oar handle force and scapula retractors during mid-drive or repetitive stress from the external oblique muscles and rectus abdominis muscle may result in stress fractures (McDonnell et al. 2011). Another hypothesis is that stress fractures are caused by co-contraction of the serratus anterior muscle and external oblique muscles. The serratus anterior muscle inserts on the anterolateral end of the 1st to 9th ribs, interweaving with the external oblique muscles. With these muscles contracting together, a downward bending stress is subjected to the ribs, mostly at the posterolateral angle, which may result in a stress fracture (Gregory et al. 2002; Lord et al. 1996; McDonnell et al. 2011). Case reports have shown increased risk of rib stress fractures associated with amenorrhea, low bone mineral density, or poor technique, in combination with errors in building training load or volume and technique (Gregory et al. 2002; Karlson 1998; McDonnell et al. 2011; McKenzie 1989). Other possible etiological factors could be joint hypomobility, vertebral malalignment, and lack of strength or flexibility (Bojanic and Desnica 1998; Christiansen and Kanstrup 1997; Holden and Jackson 1985; McDonnell et al. 2011).
Symptoms of rib stress fractures include generalized rib pain most commonly in the lateral chest region that increases with specific activity (Hickey et al. 1997; Warden et al. 2002). The pain gets worse with activity and better with rest and may be worsened by deep breaths, coughing, using the arm overhead, or due to pressure on the affected region by lying in lateral position. Physical examination reveals tenderness directly over the affected rib and sometimes with compression of the thorax.
13.3.3 Fracture of the Sternum
Fractures of the sternum mostly result from a direct high-energy trauma in vehicle accidents, when the chest strikes the steering wheel or the dashboard. A small number of traumatic sternal fractures are caused by direct blows received during sports activities as rugby, American football, hockey, or soccer (Culp et al. 2010). The sternal fractures in this group are often accompanied by rib or spine fractures. Intrathoracic organ injury should be ruled out (Jones and Matthews 1988; Robertsen et al. 1996).
Stress fractures of the sternum occur in a minority of cases (0.5 % of sternal fractures) (Buckman et al. 1987) and have a distinctly different pathogenesis. This rare condition may result from extreme upper body stresses, such as in wrestling (Keating 1987), or due to repetitive hyperflexion of the thorax, as in performing prolonged, strenuous “sit-up” exercises (Robertsen et al. 1996). Sternal stress fractures have also been reported in military recruits performing triceps dips and in a golf player (Barbaix 1996; Hill et al. 1997). Sternal insufficiency fractures occur in patients with risk factors for decreased bone density, such as osteoporosis, and in postmenopausal women. Sternal insufficiency fractures should therefore be considered in the differential diagnosis of chest pain in female athletes at risk for the female athlete triad (eating disorders, amenorrhea/oligomenorrhea, and decreased bone mineral density) (Horikawa et al. 2007; Huang et al. 2012).
The athlete suffering a sternal stress (fatigue and insufficiency) fracture complains of anterior chest pain, usually aggravated by movement and deep breathing. The onset of complaints may be gradual or sudden. History may reveal a sudden increase in upper body or abdominal training. On physical examination tenderness over the sternum or manubrium on palpation is found, sometimes accompanied by local swelling.
The etiology of sternal stress fractures has not been completely elucidated. Repetitive traction of surrounding muscles is thought to play an important role. The sternocleidomastoid muscle and the pectoralis major are attached anteriorly to the manubrium and sternum, the sternohyoid and sternothyroid muscles are attached to the posterior surface, and the rectus abdominis muscle is attached to the distal end of the sternum. Repetitive traction of these muscles may transmit forces on to the sternum, which eventually exceed the elasticity of the bone resulting in a stress fracture (Gregory et al. 2002).
13.3.4 Sternoclavicular Joint Disorders
The sternoclavicular joint is a diarthrodial, saddle-type joint. It is the only true articulation between the clavicle of the upper extremity and the axial skeleton via the sternum (Spencer et al. 2007). The articular surface of the medial clavicle is significantly larger than the sternal articular surface; less than half of the medial clavicular surface articulates with the upper angle of the sternum. Both articular surfaces in the sternoclavicular joint are covered with fibrocartilage, and between these surfaces an articular disk is interposed. Because of its anatomy, the sternoclavicular joint is characterized by the least bony stability of all major joints in the body (Brukner and Khan 2012; Spencer et al. 2007). The integrity of the joint is provided by the surrounding ligaments: the intra-articular disk ligament, costoclavicular ligament, capsular ligaments, and interclavicular ligament (Fig. 13.2). As a result of this strong stabilization, a large energy vector is required to disrupt the articulation (Martetschläger et al. 2013). Injuries to the sternoclavicular joint in athletes are consequently very rare. The incidence of sternoclavicular injuries in the normal population, based on a report of 1,603 injuries around the shoulder girdle, was 3 % (Bontempo and Mazzocca 2010; Rowe and Marble 1958; Spencer et al. 2007).
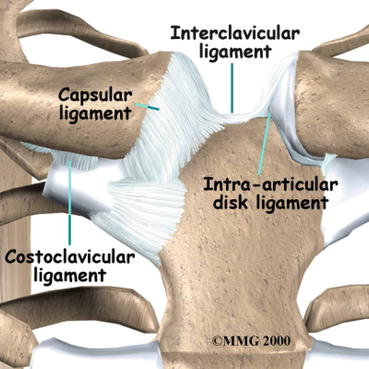
Fig. 13.2
Ligamentous anatomy surrounding the sternoclavicular joint.Courtesy: Medical Multimedia Group LLC
Although spontaneous subluxations have been reported, injuries to the sternoclavicular are often caused by a direct trauma or, more commonly, indirectly from a trauma to the shoulder. The most common cause of traumatic subluxations or dislocations of the sternoclavicular joint is traffic accidents. Injuries caused by participation in contact sports are less common (Asplund and Pollard 2004; Marker and Klareskov 1996; Pearsall and Russell 2000; Perron 2003). Simultaneous injuries of the acromioclavicular and sternoclavicular joints are common (Brukner and Khan 2012). Traumatic injuries of the sternoclavicular joint can be divided into mild sprain, moderate sprain (subluxation), or severe sprain (dislocation) and fractures of the medial clavicle physeal growth plate in adolescents and young adults. In a mild sprain the ligaments are intact and the joint remains stable. In a moderate sprain the joint capsule and ligaments may be partially ruptured along with subluxation of the sternoclavicular joint. In a severe sprain there is a disruption of the sternoclavicular ligaments, caused by dislocation. The majority of the displacements occur in an anterior or posterior direction (Brukner and Khan 2012; Spencer et al. 2007). Anterior displacements are more common; posterior displacements are potentially more dangerous because of the closed proximity of vital structures posterior to the joint, including the subclavian artery and veins, the trachea and esophagus, and the mediastinum (Brukner and Khan 2012).
Subluxation or dislocation of the sternoclavicular joint is also seen without any history of trauma. The vast majority of spontaneous or atraumatic dislocations are anterior. Spontaneous subluxations and dislocations occurring when the patient raises the arms to the overhead position are mostly associated with generalized ligamentous laxity (Spencer et al. 2007).
Another cause of complaints to the sternoclavicular joint is osteoarthritis, for which postmenopausal women, patients with chronic instability, and manual laborers are at a higher risk. Although primary degenerative osteoarthritis of the sternoclavicular joint is common after capsular or ligamentous injuries, moderate to severe changes of the joint were also found in 50 % of individuals aged over 60 years in a postmortem study. It is unknown whether these changes were posttraumatic in nature or resulted from aging (Iannotti and Williams 1999; Martetschläger et al. 2013).
In the assessment of sternoclavicular dislocations beneath 25 years of age, a fracture through the physeal plate should be considered as cause, because the medial clavicular epiphysis is the last epiphysis in the body to ossify (around the 18th to 20th year of life) and fuse (during the 23rd to 25th year) (Brukner and Khan 2012; Franck et al. 2003; Leighton et al. 1989; Lewonowski and Bassett 1992; Sferopoulos 2003; Spencer et al. 2007; Yang et al. 1996; Zaslav et al. 1989).
Depending on the severity of the injury, patients with sprain and displacement of the sternoclavicular joint present with a sharp local pain (particularly with movements of the arm) and swelling. Patients with posterior dislocations have more pain than in an anterior dislocation. The athlete usually supports the injured arm across the trunk with the normal arm. Examination reveals local tenderness with palpation and when the shoulders are pressed together by lateral pressure. In a posterior dislocation the medial end of the clavicle is less prominent and visible and palpable when compared with the normal side. Damage to the underlying vital structures should be considered when a posterior dislocation is suspected (Brukner and Khan 2012; Spencer et al. 2007).
In chronic symptoms of the sternoclavicular joint, Tietze’s syndrome, aseptic necrosis of the medial end of the clavicle (Friedrich’s disease), SAPHO syndrome, condensing osteitis, and sternocostoclavicular hyperostosis should also be considered (Martetschläger et al. 2013; Spencer et al. 2007).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


