Childhood transverse myelitis is an acute inflammatory disorder of the spinal cord with a risk of permanent disability. A timely and accurate diagnosis is imperative, and the radiologist needs to discern between a variety of extra-axial and spinal cord abnormalities that produce similar symptoms but require vastly differing treatments. This article presents the range of imaging characteristics seen in childhood transverse myelitis and the differentiation from its mimics.
Key points
- •
Transverse myelitis presents with acute motor weakness or sensory deficits, usually accompanied by bladder or bowel incontinence. These symptoms evolve over hours to days.
- •
Determining a clinical “spinal cord level” aids the planning of spinal cord imaging.
- •
Adequate spinal cord imaging requires good-quality magnetic resonance imaging with a minimum of T2-weighted sequences in 2 planes.
- •
Mimics such as tumors, epidural abscess, arteriovenous malformation, and compressive bone disease may require urgent intervention.
Introduction
Transverse myelitis (TM) is a monophasic, likely postinfectious, inflammatory disorder of the spinal cord. In some children, TM may represent the first clinical event of a chronic demyelinating disorder such as multiple sclerosis (MS) or neuromyelitis optica (NMO). Diagnostic criteria requires signs and symptoms attributable to the spinal cord, that is, sensory, motor, or bladder and bowel dysfunction, with progression to nadir in less than 21 days from onset, and cerebrospinal fluid (CSF) or neuroimaging evidence of spinal cord inflammation.
A variety of extra-axial and spinal cord disorders gives rise to acute and subacute signs and symptoms in the spinal cord. This article describes the clinical and radiologic features of TM and its mimics ( Box 1 ).
Extra-axial Compression, Disease
- 1.
Vertebral spine disorders
- a.
Trauma
- b.
Atlantoaxial subluxation
- i.
Trisomy 21
- ii.
Mucopolysaccharidosis type IV
- iii.
Grisel syndrome
- i.
- c.
Destructive lesions
- i.
Tuberculosis
- ii.
Lymphoma
- iii.
Langerhans cell histiocytosis
- i.
- d.
Scheuermann disease
- a.
- 2.
Epidural disease
- a.
Tumor
- i.
Neuroblastoma
- ii.
Wilms tumor
- i.
- b.
Abscess
- i.
Associated dermal sinus, vertebral body infection
- i.
- a.
- 3.
Arachnoiditis
- a.
Tuberculosis
- b.
Cryptococcosis
- c.
Carcinomatous infiltration
- a.
- 4.
Spinal nerve root inflammation
- a.
Guillain-Barré syndrome
- a.
Spinal Cord Disorders
- 1.
Congenital malformation
- a.
Neurenteric cysts
- b.
Spinal cord tethering
- a.
- 2.
Infection
- a.
Nonpolio enteroviruses
- b.
West Nile virus
- c.
Human T-lymphocyte virus 1
- d.
Neurocysticercosis
- a.
- 3.
Vascular disorders
- a.
Arteriovenous malformation
- b.
Cavernomas
- c.
Cobb syndrome
- d.
Fibrocartilaginous embolization
- e.
Spinal cord infarction
- a.
- 4.
Vasculitis
- a.
Systemic lupus erythematosus
- b.
Behçet disease
- a.
- 5.
Nutritional disorders
- a.
Vitamin B12 deficiency
(Subacute combined degeneration)
- a.
- 6.
Toxic injury
- a.
Chemotherapy (eg, methotrexate)
- a.
Acute deficits constitute a medical emergency requiring urgent spinal imaging, as vascular disorders and spinal cord compression have a time-sensitive relationship of treatment to outcome. In TM, a rapid evolution of symptoms usually signifies more severe disease.
Introduction
Transverse myelitis (TM) is a monophasic, likely postinfectious, inflammatory disorder of the spinal cord. In some children, TM may represent the first clinical event of a chronic demyelinating disorder such as multiple sclerosis (MS) or neuromyelitis optica (NMO). Diagnostic criteria requires signs and symptoms attributable to the spinal cord, that is, sensory, motor, or bladder and bowel dysfunction, with progression to nadir in less than 21 days from onset, and cerebrospinal fluid (CSF) or neuroimaging evidence of spinal cord inflammation.
A variety of extra-axial and spinal cord disorders gives rise to acute and subacute signs and symptoms in the spinal cord. This article describes the clinical and radiologic features of TM and its mimics ( Box 1 ).
Extra-axial Compression, Disease
- 1.
Vertebral spine disorders
- a.
Trauma
- b.
Atlantoaxial subluxation
- i.
Trisomy 21
- ii.
Mucopolysaccharidosis type IV
- iii.
Grisel syndrome
- i.
- c.
Destructive lesions
- i.
Tuberculosis
- ii.
Lymphoma
- iii.
Langerhans cell histiocytosis
- i.
- d.
Scheuermann disease
- a.
- 2.
Epidural disease
- a.
Tumor
- i.
Neuroblastoma
- ii.
Wilms tumor
- i.
- b.
Abscess
- i.
Associated dermal sinus, vertebral body infection
- i.
- a.
- 3.
Arachnoiditis
- a.
Tuberculosis
- b.
Cryptococcosis
- c.
Carcinomatous infiltration
- a.
- 4.
Spinal nerve root inflammation
- a.
Guillain-Barré syndrome
- a.
Spinal Cord Disorders
- 1.
Congenital malformation
- a.
Neurenteric cysts
- b.
Spinal cord tethering
- a.
- 2.
Infection
- a.
Nonpolio enteroviruses
- b.
West Nile virus
- c.
Human T-lymphocyte virus 1
- d.
Neurocysticercosis
- a.
- 3.
Vascular disorders
- a.
Arteriovenous malformation
- b.
Cavernomas
- c.
Cobb syndrome
- d.
Fibrocartilaginous embolization
- e.
Spinal cord infarction
- a.
- 4.
Vasculitis
- a.
Systemic lupus erythematosus
- b.
Behçet disease
- a.
- 5.
Nutritional disorders
- a.
Vitamin B12 deficiency
(Subacute combined degeneration)
- a.
- 6.
Toxic injury
- a.
Chemotherapy (eg, methotrexate)
- a.
Acute deficits constitute a medical emergency requiring urgent spinal imaging, as vascular disorders and spinal cord compression have a time-sensitive relationship of treatment to outcome. In TM, a rapid evolution of symptoms usually signifies more severe disease.
Anatomic considerations in spinal cord disorders
The spinal cord consists of 31 segments: 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 1 vestigial coccygeal segment. These segments map to respective clinical myotomes and dermatomes, and are named according to their level of supply, thus the 8 pairs of spinal nerves arising from the cervical segment are called C1 to C8. The anatomic location of the spinal cord segments do not correspond to the vertebral bodies that make up the vertebral canal. Almost all of the spinal cord itself rests in the cervical and thoracic regions of the vertebral column; only the sacral segments reside in the upper 2 lumbar vertebrae. As there are only 7 cervical vertebrae, the first 7 cervical nerve roots exit in the intervertebral foramina above their respective vertical bodies, and the C8 nerve exits below the seventh cervical vertebra. The thoracic (T1–T12), lumbar (L1–L5), and sacral (S1–S5) nerves exit below their respective vertebrae ( Fig. 1 ).
The descending corticospinal and ascending sensory tracts in the spinal cord are arranged in longitudinal bundles and are oriented with the lower body and leg regions situated medially. These considerations are important in planning spinal cord imaging, especially in hospitals in resource-limited regions, or when imaging of the entire spinal cord may not be possible. A patient with motor and sensory deficits mapping to the lower lumbar and sacral spinal cord segments will first require careful imaging of the spinal cord residing in the lower thoracic–lumbar vertebral region. A negative study will then prompt the evaluation of the cervical and upper thoracic regions.
Technical aspects of spinal cord imaging
Acute spinal cord neurologic signs and symptoms that trigger an MR imaging request should have sequences targeted to assess the spinal cord. For this reason the authors image with standard spin-echo or fast spin-echo (FSE) T1-weighted and T2-weighted sequences, usually in 2 planes. The standard imaging protocol would include sagittal and axial T2-weighted sequences throughout the spinal column followed by sagittal T1-weighted sequences precontrast in most circumstances. If a lesion is seen in the cord, postgadolinium sequences in the sagittal and axial plane will be applied. Extra sequences include thin-section axial T2-weighted sequences (targeted usually to a clinically suspected abnormal level) as well as sagittal diffusion and gradient-echo sequences to assess for cord ischemia and hemorrhage ( Table 1 ).
| Sequence | Flip Angle (°) | TR (ms) | TE (ms) | NSA | BW (Hz) | Slice/Gap (mm) | FOV (mm) | Pixel (mm) |
|---|---|---|---|---|---|---|---|---|
| Sag T2 TSE | 90 | 2500 | 130 | 4 | 180 | 3/0.5 | 280 | 0.5 × 1 |
| Sag T1 TSE | 90 | 525 | 10 | 4 | 280 | 3/0.5 | 280 | 0.5 × 1.25 |
| Ax T2 TSE | 90 | 4775 | 130 | 4 | 186 | 3/0.5 | 150 | 0.5 × 0.5 |
| Ax T1 TSE | 90 | 603 | 13 | 4 | 322 | 5/7.5 | 150 | 0.8 × 0.9 |
| Ax T2 FFE (MPGR) | 20 | 720 | 23 | 2 | 108 | 4/0.5 | 150 | 0.6 × 0.6 |
It is important to discuss with the referring neurologist the clinical presentation. If the presentation is more consistent, for example with Guillain-Barré syndrome, sequences targeting the enhancement of the nerve roots such as axial and sagittal T1-weighted scans are used.
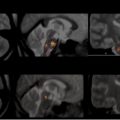
Scanning on a 1.5-T machine has been preferred to avoid multiple artifacts that occur in spinal cord imaging and which are magnified because of the higher signal-to-noise ratio with higher field magnets. However, improved pulse-sequence design has led to an increase in the use of 3 T, and advanced imaging such as diffusion tensor imaging can also be reliably obtained. Marked CSF pulsation artifact, which can obscure the cord signal from flow-related artifact, is an important artifact to consider. The body’s mean daily CSF production is 500 mL, and it has a pulsatile motion caused by the expansion and contraction of the brain and intracranial vessels associated with the cardiac cycle. This pump effect causes the CSF flow in the cervical spaces to be 40% as fast as in the carotid arteries, resulting in multiple artifacts that may appear hypointense on T2-weighted images, particularly posterior to the spinal cord, where they can be very impressive ( Fig. 2 ). Such artifacts are much more pronounced in children than in adults. Another artifact that can be a challenge is the “Gibbs or truncation artifact.” These bright or dark lines are seen parallel to edges of abrupt intensity changes, sometimes described as “ringing” artifacts following signal-intensity borders. This pattern occurs when the number of phase-encoding steps at high spatial resolution is undersampled and, hence, is unable to faithfully reproduce the true anatomic details of the original image. In addition, these artifacts may occur when the number of peripheral Fourier lines in the k-space is small or insufficient. Such artifacts are observed particularly at 3 T, as a consequence of the improved signal-to-noise ratio in comparison with 1.5-T MR imaging. Their occurrence can be reduced by either increasing the spatial resolution or applying reconstruction filters, to smoothen the signal at the edges of k-space.