Chapter 135
Chordoma
Epidemiology
Chordomas are thought to arise from the remnants of the notochord, the embryonic precursor of the axial skeleton. Chordomas are usually seen in the fifth and sixth decades but they may be found in all age groups. There is no sex predilection. Spheno-occipital chordomas account for 35% of cases and are more commonly encountered in children and the younger age group. Fifty percent of chordomas are located in the sacrococcygeal area; these tumors usually occur in the fifth and sixth decades.
Clinical Findings
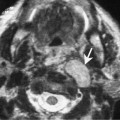
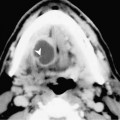
Clinical signs and symptoms depend on the size and location of the tumor. Encroachment of the neural or jugular foramen may produce cranial nerve palsy. Intracranial extension may produce signs related to brainstem compression. If the tumor extends into the nasopharynx or nasal cavity, breathing difficulty and nasal stuffiness may be the presenting symptoms.
Pathology
Grossly, they are locally invasive, soft or firm lobulated masses. There are two histologic varieties of chordomas. The regular type closely resembles normal notochord tissue in different stages of development. In typical chordomas, vacuolated physaliphorous cells with variable amounts of intracytoplasmic mucin are embedded in pools of extracellular mucin. The second variety is the chondroid type that is associated with a cartilaginous matrix.
Treatment