, Jean-Philippe Bault2, Bernard Benoit3 and Gérard Couly4
(1)
Center of women and fetal imaging, Créteil, France
(2)
Center of fetal imaging Ambroise Paré, Les Mureaux, France
(3)
Princess Grace Hospital, Monaco, France
(4)
Department of maxillo-facial surgery, Necker Hospital, Paris, France
3.1 Clefts
3.1.1 Introduction
3.1.1.1 Why screen?
Facial clefts are found in 272 different syndromes, the frequency of cleft lips and palate is 0.5/1000, or 1/500, 41 % of which are associated with other organ anomalies, and only 6/10 being isolated.
3.1.1.2 Face and Brain: The Key Combinations of Pathologies to Know
When a facial cleft is discovered, complete analysis of the face associated with a morphological diagnostic study should be done, due to the frequent association between clefts and pathological syndromes, as was confirmed in this study by Gérard Couly, done at the Necker Hospital in Paris.
There is clearly a predominant association between the face and the brain (Table 3.1).
Table 3.1
Brain malformations associated with facial malformations
Facial malformations | Brain malformations | |||
|---|---|---|---|---|
Labio-maxillary and velo-palatal and Philtrum abnormalities | 170 | Unilateral 135 | 1 lissencephaly + (epilepsy) 1 agenesis of corpus callosum | 14 |
Bilateral 35 | 10 holoprosencephaly 1 encephalocele (Meckel) 1 cortical malformation | |||
Maxillo-madibular dysplasias | 44 | Francescetti S. Goldenhar S. 1st arch S. | 1 agenesis of corpus callosum 5 posterior fossa anomalies (cyst, mega cisterna) | 6 |
Pierre Robin syndrome | 60 | 3 mega cisterna magna 1 occipital porencephaly | 4 | |
3.1.1.3 Facial Clefts and the Nose-Mouth Image During the Second and Third Trimesters, at 22 GW and 32 GW
The classic entry point for facial clefts is on the “nose-mouth” image, with analysis of the upper lip, the philtrum and below the septum.
A lip cleft is the starting point for labio-maxillary and/or palate clefts.
The second trimester report can no longer be written with such laconic sentences as “face unseen during this examination.”
Now, during the second trimester of pregnancy, one should be able to effectively screen for facial clefts, at the very least cleft lip.
3.1.2 Symptomatic Analysis of Clefts
3.1.2.1 Unilateral Cleft Lip
This is characterized by the bi-partitioning of the peri-buccal integuments and muscles and respects the gums and the dental alveoli in the upper maxilla.
It is possible to describe:
The cleft side.
The right and left processes.
The skin and mucosa on either side of the cleft, the nostril bridge and nostril asymmetry.
The seriousness of the defect on the median level and particularly at the philtrum level.
3.1.2.2 Bilateral Cleft Lip
This is characterized by the tri-partitioning of the peri-buccal integuments and muscles, and respects the gums and the dental alveoli in the upper maxilla.
It is possible to describe:
The median process, under the nostrils
The surface of the skin on the median process, and how much excess mucosa there is.
Mucosa
Skin
The two clefts on either side of the median process and their possible asymmetry.
For each side, describe as one would a unilateral labial cleft
The right and left processes
The skin surface and mucosa on either side of the cleft.
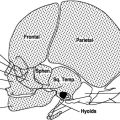
The sagittal and para–sagittal views enable one to the complete the examination with observation of related markers:
Position of the tongue
Orbits
Bone structure: zygomatic arch, malar bone.
Visualization of the soft palate.
The axial view, or more precisely the stepped axial views:
These will make it possible to see to what extent the cleft impacts the maxilla, the back side of the palate and the pterygoid apophyses, the tongue position and the mandibular arch.
3.1.2.3 What 3D Can Do
Multi–view sagittal and axial views, in TUI mode associated with thick VCI mode views.
The study of millimetric views enables the detailed analysis in three planes for possible deformations of bone structures.



Fig. 3.1
Labioalveolar-palatal cleft. Overview in three planes
Fig. 3.2
Labioalveolar-palatal cleft. Axial view
Fig. 3.3
Labioalveolar-palatal cleft. Axial view
3.1.3 Ultrasound Diagnosis of Clefts: Analytical Study
Once the diagnosis of a lip abnormality has been uncovered, the ultrasonographer must use a simple, strict diagnostic methodology:
Description of the cleft lip
Description of the cleft maxilla if there is one
Description of the cleft palate if there is one.
3.1.3.1 Analytical Study of First Trimester Clefts
On the Herman score sagittal view, the upper lip could have a comma-shaped deformation, with slight eversion of its inferior portion, which should alert the ultrasonographer that there may be a cleft lip.
The nose–mouth view can then show the defect.
Maxillary and mandibular axial views are easy to capture and can show the bi-partitioning of the facial mass if there is a labio-maxillary unilateral cleft, or a tri-partitioning in the case of a bilateral labio-maxillary cleft.
An open–mouth sagittal view is rather easy to capture for an examination targeting the palate, and enables one to follow both the hard and soft palates. The image is almost easier to capture at this stage than during the second trimester, because there are fewer shadows linked to ossification.
What 3D Can Do
Skin surfacing objectifies the processes well.
The multi-planar technique and using thick views makes it possible to capture stepped axial views starting from the orbit on to of the mandibular cavities.

Fig. 3.4
Uniliteral labioalveolar cleft at 12 GW
It is easier to look for associated anomalies during the first trimester. With trisomy 13, the associated hexadactylism can be seen in the same 3D volume, and for that reason, one must record the largest volume possible.


Fig. 3.5
Otocephaly
Fig. 3.6
Unilateral labial cleft
3.1.3.2 Analytical Study of Clefts from the 2nd Trimester
The most favorable time frame is between 20 and 25 GW.
The major types of clefts:
Unilateral cleft lip.

Fig. 3.7
Labioalveolar and palatal cleft
Unilateral labio-alveolar-palatal cleft.

Fig. 3.8
Bilateral labioaveolar-palatal cleft. 3D reconstructed views of the palate
Bilateral labio-alveolar cleft impacting the primary palate, with an intact secondary palate.

Fig. 3.9
17 GW median cleft lip – trisomy 13
Median cleft: a particular and associated pathology.

Fig. 3.10
Labioalveolar and palatal cleft, stepped axial views
3.1.3.3 Basic Principles for Obtaining 2D and 3D Views
Position of the head:
The position of the fetal head during image capture is important for precise rendering and for the diagnosis.
- 1.
A denected position is used to capture and render images of the primary and secondary palates.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree