, Joungho Han2, Man Pyo Chung3 and Yeon Joo Jeong4
(1)
Department of Radiology Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea, Republic of (South Korea)
(2)
Department of Pathology Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea, Republic of (South Korea)
(3)
Department of Medicine Division of Pulmonary and Critical Care Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea, Republic of (South Korea)
(4)
Department of Radiology, Pusan National University Hospital, Busan, Korea, Republic of (South Korea)
Abstract
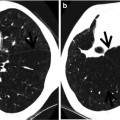
The sign has been originally described on chest radiographs. It is formed by distorted blood vessel(s) and a focal area of atelectatic lung adjacent to pleural thickening. The vessel(s) are seen as curvilinear soft tissue density or densities, extending from the medial margin of the atelectatic lung to the pulmonary hilum. When the vessels are multiple thus there are multiple tails, the vessels are more likely parachute; then, parachute sign may be used (Fig. 5.1). The sign is due to contracted fibrous scarring and shrinking pleural disease with rounded atelectasis. Likewise, on CT, swirling of bronchi and vessels extending from the hilum and converging on the atelectatic lung help produce comet tail appearance [1] (Figs. 5.1 and 5.2).
Definition
The sign has been originally described on chest radiographs. It is formed by distorted blood vessel(s) and a focal area of atelectatic lung adjacent to pleural thickening. The vessel(s) are seen as curvilinear soft tissue density or densities, extending from the medial margin of the atelectatic lung to the pulmonary hilum. When the vessels are multiple thus there are multiple tails, the vessels are more likely parachute; then, parachute sign may be used (Fig. 5.1). The sign is due to contracted fibrous scarring and shrinking pleural disease with rounded atelectasis. Likewise, on CT, swirling of bronchi and vessels extending from the hilum and converging on the atelectatic lung help produce comet tail appearance [1] (Figs. 5.1 and 5.2).
Get Clinical Tree app for offline access
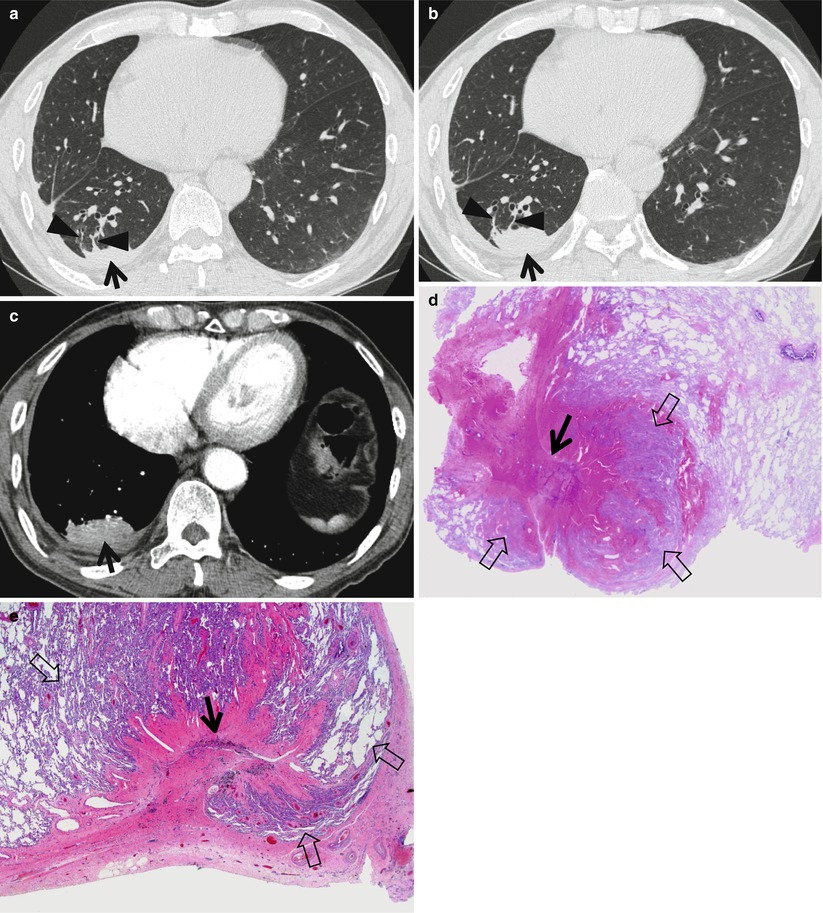
Fig. 5.1
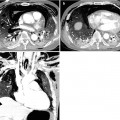
Rounded atelectasis in a 66-year-old man complaining of shortness of breath and cough. (a, b) Consecutive thin-section (1.5-mm section thickness) CT scans obtained at ventricular level show the atelectatic right lower lobe (arrows) abutting pleura. Also note two vascular curvilinear soft tissue attenuations (arrowheads), extending from anterior margin of the atelectatic lung to pulmonary hilum; these two structures may help explain parachute sign (please refer to definition of comet tail sign) on chest radiograph in this particular condition (rounded atelectasis). Also note right pleural effusion and thickening, posterior to the atelectatic lung, and extrapleural subcostal fat accumulation. (c) Mediastinal window image demonstrates the enhancing atelectatic lung (arrow) abutting pleura. (d) Low-magnification (×10) photomicrograph of pathologic specimen obtained from a different patient with rounded atelectasis depicts enfolded visceral pleura (arrow) curving into a rounded atelectatic lung that gestures wings (open arrows) of a vane. (e) High-magnification (×100) photomicrograph discloses more clearly enfolded visceral pleura (arrow




Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
