, Joon Woo Lee1 and Jong Won Kwon2
(1)
Department of Radiology, Seoul National University Bundang Hospital, Seongnam, Kyonggi-do, Republic of Korea
(2)
Department of Radiology, Samsung Medical Center, Seoul, Republic of Korea
6.2.1 Chemical Shift Artifact
6.2.3 Truncation Artifacts
6.2.4 Aliasing Artifacts
6.2.5 Motion-Related Artifacts
6.2.6 Saturation Artifact
6.3.2 Chemical Shift Artifact
6.3.4 Truncation Artifact
6.3.5 Aliasing Artifact
6.3.6 Motion-Related Artifacts
6.3.7 Saturation Artifact
Abstract
Common normal anatomic structures on spinal MR imaging potentially mimicking pathology include epidural veins, intraosseous veins, and nerve roots. Common spinal MR imaging artifacts include chemical shift artifact, susceptibility artifact due to metallic implants, truncation artifact, aliasing artifact, motion artifact, saturation artifact, artifact due to radio-frequency interference, and artifact due to incomplete fat saturation. In this chapter, we will describe the main characteristics of these entities.
Common normal anatomic structures on spinal MR imaging potentially mimicking pathology include epidural veins, intraosseous veins, and nerve roots. Common spinal MR imaging artifacts include chemical shift artifact, susceptibility artifact due to metallic implants, truncation artifact, aliasing artifact, motion artifact, saturation artifact, artifact due to radio-frequency interference, and artifact due to incomplete fat saturation. In this chapter, we will describe the main characteristics of these entities.
6.1 Common Normal Structures and Variants Mimicking Spinal Disorders on MRI
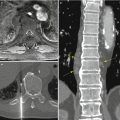
Common normal anatomic structures that may be misinterpreted as spinal disorders include epidural veins, intraosseous veins, and nerve roots. Vascular structures such as epidural and intraosseous veins can be traced and have a tubular configuration. Vascular structures were usually of lower signal than nerve roots on T1- and T2-weighted images. An epidural vein may be mistaken for a herniated disk if it is located in the anterior epidural space posterior to the disk. Findings suggestive of epidural veins include low signal on both T1- and T2-weighted images, linear configuration parallel to the nerve root, a gap between the vessel and posterior margin of disk, and tapered appearance in the neural foramen. Intraosseous veins can be mistaken for fractures because of its linear low-signal appearance. However, an intraosseous vein usually shows a tortuous course and appears as a thicker line than a fracture and contiguity can be traced to the epidural or paravertebral veins.
Nerve roots are derived from the dural sac and show variable origin, with conjoined nerve roots sometimes encountered. On T1-weighted axial images, the nerve root can be easily traced because it is surrounded by high-signal fat in the epidural space. A conjoined nerve root may be misinterpreted as a herniated disk. Occasionally, a herniated disk can severely compress upon and displace the nerve root, such that the herniated disk is situated in the usual expected location of the nerve root on axial images. In this instance, the focal herniation may be mistaken for a nerve root. Thus careful review of the sagittal MR images should be performed. Focal disk herniation compressing upon the nerve root may be demonstrated in continuity to the parent disk on sagittal images. In addition, nerve roots show intermediate signal on T1-weighted and T2-weighted images and are usually of slightly higher signal than disk herniation.
6.2 Common MR Artifacts on Spinal Imaging
6.2.1 Chemical Shift Artifact
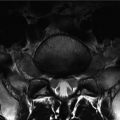
Chemical shift artifact is caused by misregistration of fat protons relative to water protons due to a small difference in precessional frequencies (approximately a difference of 224 Hz at 1.5 T). Chemical shift artifact is produced at the interface between water and fat along the frequency-encoding direction. Chemical shift artifact is manifested as hyperintense areas where fat and water signals overlap and as hypointense areas where fat and water signals separate (Soila et al. 1984; Peh and Chan 2001).
6.2.2 Susceptibility Artifacts Due to Metallic Implants
Susceptibility artifacts due to metallic implants are produced by the large differences in magnetic properties between human tissues and implanted metals, creating local magnetic field inhomogeneities altering the phase and frequency of local spins. This results in distortion of the shape of the metallic object along the frequency-encoding and section selection axes, as well as loss of signal within the metallic object. A rim of high signal intensity appears around the metallic object as a result of mismapping of a disproportionate number of spins to that location. Titanium implants produce much less severe artifacts than stainless steel, while larger implants produce more artifacts. When the direction of the main magnetic field (z axis of the MR scanner) is aligned parallel with the longitudinal axis of the hardware device, there is a significant relative reduction in artifacts (Suh et al. 1998; Frazzini et al. 1997). Gradient-recalled echo (GRE) sequences are extremely sensitive to the presence of metal compared to spin echo sequences, and higher field strength MRIs show more severe susceptibility artifact. Susceptibility artifacts due to metal may be exaggerated on fat-saturated sequences as well.
6.2.3 Truncation Artifacts
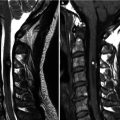
Truncation artifacts are manifest as bright or dark lines seen parallel and adjacent to borders of abrupt intensity change, for example, at the interface between bright CSF and the low-signal spinal cord on T2-weighted images (Czervionke et al. 1988). On sagittal images, a central stripe within the spinal cord due to truncation artifact may mimic spinal cord pathology such as a syrinx; a fine linear signal along the spinal cord is considered to be related to truncation artifact and not representative of true pathology.
6.2.4 Aliasing Artifacts
Aliasing artifact results in folding or wraparound of part of the structure of interest to the opposite side of the image. This occurs when the field of view used is too small, causing the phase-encoded signal outside the field of view to be superimposed inside the field of view on the opposite side. Aliasing artifacts can be eliminated through oversampling, using surface coils, increasing the field of view, or by switching the frequency- and phase-encoding directions (Morelli et al. 2011).
6.2.5 Motion-Related Artifacts
Motion is a common cause of artifacts in MR imaging. Random motion causes image blurring with decreased definition of anatomic structures. Involuntary motion due to respiration, swallowing, or bowel peristalsis produces motion artifacts resulting in imaging blur. Motion artifact is seen along the phase-encoding direction. Respiratory motion artifact is a problem in thoracic spine MR, and swallowing can cause motion artifacts in imaging of the cervical spine.
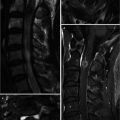
Periodic motion such as cardiac pulsation results in “ghost artifacts,” manifest as replicas of the pulsating structure in an abnormal but predictable location along the phase-encoding direction (Peh and Chan 2001). The number, position, and brightness of these periodic ghost artifacts depend on the amplitude and frequency of pulsation. The brightness of the ghost artifact is proportional to the amplitude and speed of the motion. A series of bright ghost images propagating parallel to the phase-encoding direction can overlie the hypointense spinal cord, thus mimicking pathology (Wood and Henkelman 1985).
Motion can also be turbulence in the blood or CSF. Such motion results in a mixture of increased and decreased signal intensity (Taber et al. 1998). In the upper thoracic spine, the subarachnoid space posterior to the spinal cord is wide, and CSF flow artifact is common in this area. Turbulent CSF flow artifacts are seen as areas of low signal intensity on T2-weighted images and high signal intensity on T1-weighted images. On fat-suppressed postcontrast T1-weighted images, relatively high-signal CSF flow artifacts may be misinterpreted as enhancing pathology, and comparison with precontrast T1-weighted images is important. CSF flow artifact can be reduced by employing gradient-recalled echo or 3D fast spin echo imaging.
Motion can also be continuous, as with blood flowing within a vessel, resulting in a flow void on spin echo images (because the blood has moved out of the imaging volume before signal acquisition) or increased signal on gradient-recalled echo images (due to the inflow of new blood).
6.2.6 Saturation Artifact
Saturation (cross-talk) artifact is an artifact appearing as a band of signal loss when different angled axial image stacks of the spine are obtained simultaneously (Peh and Chan 2001; Taber et al. 1998). When the RF pulse excites the slice, the overlapping portion of the adjacent slice is simultaneously excited, causing the overlapped portion to be saturated and resulting in an area of decreased signal. This artifact is common in lumbar spine MRI because stacks of angled axial images are acquired at each disk level.
6.2.7 Artifacts Due to Radio-Frequency Interference
Artifact due to radio-frequency interference is seen as a linear band across the image perpendicular to the frequency-encoding direction. The possible sources of radio-frequency interference include television, radio, fluorescent lights, and electric motors (Taber et al. 1998).
6.2.8 Artifacts Due to Incomplete Fat Saturation
Artifacts due to incomplete fat saturation can be seen in cases of selective fat suppression employing frequency-selective pre-saturation to eliminate unwanted signal from fat. These types of artifacts can be caused by (1) magnetic susceptibility difference between fat and air or (2) magnetic field inhomogeneity in large fields of view. These can be seen as an area of either brighter signal (poor saturation) of the fat or dark signal (incorrect suppression of water signal) of normal tissues.
Table 6.1
Spinal MR artifacts
Artifact | Findings |
|---|---|
Chemical shift artifact | Hyperintense areas where fat and water signals overlap and hypointense areas where fat and water signals separate |
Susceptibility artifacts due to metallic implants | Distortion of the shape of the metallic object with loss of signal within |
Rim of high signal intensity around the metallic object | |
Truncation artifacts | Bright or dark lines parallel and adjacent to borders of abrupt intensity change |
A central high-signal stripe in the cord due to truncation artifact may mimic a syrinx | |
Aliasing artifacts | Phase-encoded signal outside the field of view superimposed inside the field of view on the opposite side |
Periodic motion such as cardiac pulsation | “Ghost artifacts” replicate the pulsating structure in an abnormal but predictable location along the phase-encoding direction |
Involuntary motion due to respiration, swallowing, or bowel peristalsis | Image blur |
Turbulent motion like cerebrospinal fluid | Mixture of increased and decreased signal intensity
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|