Risk assessment
Hemodynamic emergencies
Aortic annulus
Aortic root and coronary arteries
Aortic root morphology
Ectopic calcification
Wire position
Mitral valve apparatus
Left ventricular size and function
Balloon aortic valvuloplasty
Positioning and deployment of THV
Aortic valve, root, and LVOT morphology
Aortic/AV trauma
Periaortic hematoma
Aortic dissection
Annular rupture
Pericardial tamponade
Mitral valve compromise
Left main coronary occlusion
Severe aortic regurgitation
Central regurgitation
Paravalvular regurgitation
Confirmation of Wire and Catheter Placement
TEE can be used to confirm placement of catheters and wires. Central monitoring catheters placed into the right heart may require imaging during initial internal jugular puncture and insertion of the catheter into the right heart (Fig. 29.1) as described in recent guidelines [4]. Placement of the pacing wire from either superior vena caval or inferior vena caval sites may also require imaging to confirm positioning and document the presence of pericardial effusions.


Fig. 29.1
Imaging of the right internal jugular vein for placement of central monitoring catheters may require vascular imaging as well as transesophageal (TEE) imaging. (a) shows the short-axis view of the right internal jugular vein (IJV) and carotid artery (CA). (b) shows the needle (yellow arrows) causing compression (red arrows) of the vein just prior to entering the lumen. (c) shows TEE imaging of the bicaval view to confirm the entrance of the J-wire (yellow arrows) into the superior vena cava (blue arrow) and right atrium (RA). LA = left atrium
Numerous potential access sites exist for TAVR, and the function of TEE may change with the TAVR approach. For transapical TAVR, because of the small apical window generated by limited thoracotomy, imaging of the left ventricular apex (mid-esophageal view) is useful to ensure optimal location of the apical puncture (Fig. 29.2). A cannulation site in the anterior or anterolateral apex allows for appropriate axial alignment of the initial puncture and wire direction. This is important to avoid entanglement of the wire in the mitral apparatus and position the wire quickly across the aortic valve. Frequently, the location of the apical puncture is dictated by the coronary artery anatomy or abnormal positioning of the heart relative to the thoracotomy. In addition, very small, concentrically hypertrophied, and hyperdynamic ventricles may be particularly problematic. In these patients, problems may not become evident until the larger transcatheter heart valve (THV) and guide catheter are introduced. The size of the device within the small, hyperdynamic ventricle may increase the likelihood of entrapment of a left ventricular mitral chordae. During needle insertion, advancement of the guide wire, and subsequent apical cannulation, imaging of the mitral valve either with color-compare mode or biplane imaging with color Doppler may allow early recognition of valvular compromise (Fig. 29.3).


Fig. 29.2
For the transapical approach, localization of the left ventricular apex (mid-esophageal view) is performed using simultaneous multiplane imaging to ensure optimal location of the apical puncture. The yellow arrow indicates the surgeon’s digit at the proposed site of puncture
Fig. 29.3
Simultaneous two-dimensional and color Doppler imaging of the mitral valve showing tethering of the mitral leaflet (yellow arrow) caused by entrapment of stiff wire following apical cannulation. The color Doppler image suggests severe mitral regurgitation which was not seen at baseline
Mitral for the more commonly used transfemoral approach, echocardiographic imaging is used for assessing the position and stability of the J-wire within the ventricle. The stability of the wire is integral to maintaining appropriate positioning and stabilization of the transcatheter heart valve deployment catheters. The wire should be well within the body of the ventricle and a curve formed within the apex. If the wire is in the mid-ventricle (Fig. 29.4a) or wrapped around mitral chordae, the proceduralists performing TAVR will frequently reposition. 3D imaging may help localize the cannulation site and guide wire path within the ventricle (Fig. 29.4b).

Fig. 29.4
For the transfemoral approach, echocardiographic imaging is used for assessing the position and stability of the J-wire within the ventricle. Panel (a) is a biplane image of the J-wire in the mid-ventricle which is a suboptimal position. Three-dimensional imaging (panel b) may be helpful in identifying wire position as well as the relationship to the mitral valve apparatus. Arrows in both panels are pointing to the J-wire
Balloon Aortic Valvuloplasty
Balloon aortic valvuloplasty (BAV) is performed prior to TAVR to increase cusp opening and excursion and to facilitate placement of the THV. BAV however is not without complications, with serious adverse events reported in up to 15.6 % of patients [5]. These may include death, stroke, coronary occlusion, severe aortic regurgitation, resuscitation, cardioversion, tamponade, permanent pacemaker, and severe vascular complications. Echocardiography can be important in assessing the presence of aortic regurgitation and the integrity of the aorta. Acute severe aortic regurgitation may cause severe hemodynamic compromise and necessitate urgent valve implantation. Both valve avulsion (Fig. 29.5) and fixation of the markedly calcified cusps may occur. During BAV, the biplane mode is again utilized with imaging of the mid-esophageal LAX and SAX views of the AV. Following BAV, increase in cusp motion is expected and the severity of AR should be assessed. Although not routinely performed, deep transgastric Doppler can show a reduction in the transsystolic gradient (Fig. 29.6).

 Transcatheter Aortic Valve Replacement: Current Evidence from Large Multicenter Registries
Transcatheter Aortic Valve Replacement: Current Evidence from Large Multicenter Registries
 Positron Emission Tomography Evaluation of Aortic Stenosis
Positron Emission Tomography Evaluation of Aortic Stenosis
 Pathologic Findings in Aortic Stenosis
Pathologic Findings in Aortic Stenosis
 Transcatheter Aortic Valve Replacement in Patients with Chronic Kidney Disease: Pre-procedural Assessment and Procedural Techniques to Minimize Risk for Acute Kidney Injury
Transcatheter Aortic Valve Replacement in Patients with Chronic Kidney Disease: Pre-procedural Assessment and Procedural Techniques to Minimize Risk for Acute Kidney Injury
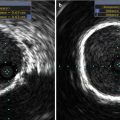 Aortoiliofemoral Angiography and IVUS
Aortoiliofemoral Angiography and IVUS
 Valve-in-Valve for Transcatheter Aortic Valve Replacement: Do Imaging Requirements Change?
Valve-in-Valve for Transcatheter Aortic Valve Replacement: Do Imaging Requirements Change?




Related posts:
Transcatheter Aortic Valve Replacement: Current Evidence from Large Multicenter Registries
Positron Emission Tomography Evaluation of Aortic Stenosis
Pathologic Findings in Aortic Stenosis
Transcatheter Aortic Valve Replacement in Patients with Chronic Kidney Disease: Pre-procedural Assessment and Procedural Techniques to Minimize Risk for Acute Kidney Injury
Aortoiliofemoral Angiography and IVUS
Valve-in-Valve for Transcatheter Aortic Valve Replacement: Do Imaging Requirements Change?
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
