CHAPTER 80 Computed Tomographic Angiography
Clinical Techniques
DSA remains the gold standard method for evaluation of atherosclerosis within the vasculature; however, this is a minimally invasive technique with the potential for iatrogenic complications. Therefore, noninvasive imaging methods are desirable among patients and physicians alike. With the advent of MDCT, noninvasive angiography has become a viable option as a result of increased speed, spatial resolution, and volume coverage. CTA revolutionized vascular imaging when vessels smaller than 1 mm in diameter were imaged with single-slice spiral CT.1–5 However, because of the small volume of coverage and limitations in the speed of image processing, CTA did not become widely used until the introduction of MDCT in 1998.6–8 With the advent of MDCT, temporal and spatial resolution of the scanners significantly improved.9,10 Gantry rotation times of 0.28 to 0.5 second with slice thickness of 0.33 to 0.75 mm are now available on most MDCT scanners.
With MDCT, there are several parallel detectors along the z-axis, and multiple channels of data (currently up to 320) significantly improve z-axis resolution. This allows isotropic resolution for most vascular applications with images obtained during a single short breath-hold. The result has been elimination of the tradeoff between spatial resolution (z-axis) and scanning range, an important limitation of single-detector spiral CT.11,12 Hence, a significant benefit has been a paradigm shift from single-slice to volumetric data acquisition. This, in turn, has made imaging of different vascular phases with a single bolus of contrast material a reality.7 Isotropic data sets allow three-dimensional reconstruction and a variety of postprocessing methods to enable both diagnostic interpretation and eloquent anatomic and pathologic arterial display.
The advantages of CTA include lower cost and the ability to potentially reduce the total volume of contrast material administered. With the fastest scanners currently available, abdominal CTA can be performed with as little as 50 mL of contrast material with the use of saline flush.13,14 This requires meticulous attention to the timing of bolus administration of the contrast material, which is discussed later in this chapter. In evaluation of life-threatening vascular disease, such as traumatic aortic injury or pulmonary embolus, CTA has a clear advantage because of short acquisition times.15
Increased utility of CT has led to significant increase in radiation exposure and concerns about its effect.16 CT currently accounts for approximately 75% of the total radiation dose delivered by medical imaging.17 Development of automatic tube current modulation software that is now available on all advanced MDCT systems has been a positive side effect of this awareness. Tube current modulation automatically adjusts the current during scanning to decrease the amount of radiation in anatomic regions that do not require higher current (e.g., lung bases or above the iliac crest) while maintaining image quality.16 In the appropriate setting, CTA may be performed with a reduced kilovoltage setting to decrease radiation to the patient and to improve signal-to-noise ratio.18
TECHNICAL REQUIREMENTS
Technical Components and Design
Image Quality
Factors affecting image quality and characteristics of CTA images include temporal and spatial resolution. Spatial resolution refers to the degree of blurring in the image and the ability to discriminate objects and structures of small size. Axial resolution within the scan plane can be improved by using a small field of view, larger matrix size, smaller focal spot, and smaller detectors. The demand for high spatial resolution to visualize the various coronary segments that course with decreasing diameter to the apex is high. One of the major goals of MDCT technology development has been to obtain similar spatial resolution in all directions, also expressed as isotropic spatial resolution.19 CTA requires high spatial resolution to enable accurate detection and interrogation of small arterial branch vessels. Both in-plane and through-plane spatial resolutions are important indices that require optimization to provide isotropic source data. Isotropic means that the spatial resolution is approximately equal in all planes, which is necessary to enable multiplanar image reconstruction after acquisition. Isotropic data avoid loss of spatial resolution in one plane and reduce partial volume effects after source data reconstruction.20 The increased scanner detector numbers has allowed increased through-plane spatial resolution as the detector width is reduced with increased numbers (1 to 1.25 mm with 4-detector row CT, 0.5 to 0.625 mm with 64-detector row CT).21 The new MDCT scanners have not improved in-plane spatial resolution; this is determined by detector geometry and the convolution kernel (reconstruction algorithm).20 Temporal resolution is defined as the required time for data acquisition per slice. It represents the length of the reconstruction window during each heart cycle, which is determined by the gantry speed.
Detectors
Diagnostic performance in coronary CTA is primarily determined by temporal resolution, which is the required time for data acquisition per slice. The determinant of this is the gantry rotational speed. For the typical setup of a single tube and detector, half a gantry rotation is necessary to acquire the data for volume reconstruction, that is, temporal resolution is equal to half gantry rotation. The temporal resolution of a 64-slice CT scanner with a gantry rotation of 330 ms is 166 ms. For motion-free images to be obtained at any phase in the cardiac cycle, a temporal resolution of 10 ms is required. Achievement of such high temporal resolution is impossible with CT. As a result, cardiac CT phase reconstruction is centered on the quiescent or low-motion window in end-diastole. The postulated required temporal resolution for reliable cardiac imaging is in the range of 65 ms.22 One manufacturer has developed a 256-slice CT scanner (128 × 0.625) with a rotation time of 270 ms and temporal resolution of 135 ms. However, with automatic multisegmental reconstructions with voxel-based optimization, temporal resolutions up to 68 ms are achieved.
Image Acquisition and Reconstruction
Prospective Gating
Hsieh and coworkers23 have developed a new approach for CTA referred to as prospectively gated axial. This technique uses a combined step-and-shoot axial data acquisition and an incrementally moving table with prospective adaptive ECG triggering. This method takes advantage of the large-volume coverage available with the 64-slice MDCT scanner that enables complete coverage of the heart in two or three steps. With this technique, the table is stationary during the image acquisition. It then moves to the next position for another scan initiated by the subsequent cardiac cycle. The result is very little overlap between the scans, significant (50% to 80%) reduction in radiation dose, and more robust and adaptive ECG gating. Earls and associates24 reported an effective dose for the prospectively gated axial group (mean, 2.8 mSv) that was significantly lower than that for the retrospectively gated helical group (mean, 18.4 mSv). This represents a reduction in mean effective dose to the patient by up to 80% from the retrospectively gated helical to the prospectively gated axial approach.
Contrast Detection and Administration
With shortened acquisition times of MDCT, optimization and maximization of vascular enhancement have become more challenging.25,26 CTA requires excellent contrast enhancement of the targeted vessels. A good-quality CT angiogram requires an arterial density value of greater than 200 HU.27,28 This should be achieved rapidly, and the peak should coincide with the acquisition interval. It is therefore crucial to time the contrast bolus correctly. However, rapid administration of contrast material shortens the plateau phase of contrast enhancement, thus creating further challenge for correct timing of the study.25,26,29 For most CTA applications, an injection rate of 4 to 5 mL/sec yields optimal vascular enhancement.
Several factors affect time to peak from the start of contrast bolus administration. These include the iodine content of the contrast material, the injection rate, and the patient’s cardiac status.25,26,30,31 A faster injection rate, for example, can achieve a higher density in the targeted vessel and results in a higher quality CT angiogram. It also separates the arterial from the portal venous phase and hence results in excellent image quality without cross-contamination by different phases.25 Contrast material with higher iodine concentration improves vascular enhancement if all other parameters are held constant.25,32 An important consideration with the 16- and 64-slice scanners is the possibility of “outrunning” the contrast bolus in patients with low cardiac output or in cases that require long z-axis coverage (e.g., combination of extremity and abdominal CTA); to overcome this issue, one can slow down the scanner by increasing the gantry rotation time and slowing the table speed.33,34
Fixed Scan Delay
Few authors currently use the method of setting a standard timed scan delay after the intravenous administration of contrast material to acquire images in the arterial phase.35,36 By setting the same scan delay for every patient, one is assuming that exactly the same hemodynamic conditions exist in all patients. This method does not accommodate patients with any variation from the normal (i.e., low blood pressure, low cardiac outputs, hypovolemia, high outputs). We would not agree with employing this method of a fixed scan delay time.
Bolus Tracking
To more accurately determine the optimal scan delay after intravenous administration of contrast material in patients with variable hemodynamics, the technique of contrast bolus tracking can be employed. Used by many authors,37,39 this is an efficient way to optimize arterial opacification. Initially, a single low-dose CT image is obtained, without administration of contrast material, at the level of the common carotid for the carotids, the ascending aorta for the coronary and thoracic aorta, and the celiac axis for the abdominal aorta and runoffs. A 10- to 15-mm2 circular region of interest is placed inside the middle of the aortic lumen, and this will subsequently measure the Hounsfield units of the aortic lumen on subsequent scanning. At 8 to 10 seconds after intravenous administration of contrast material, serial low-dose monitoring CT scans are obtained at the same table position at 1-second intervals. When the region of interest detects a preset contrast enhancement level (usually 100 to 150 HU value), there is automatic triggering of the scanner to acquire images in the desired scan range. This time-efficient method ensures optimal arterial enhancement within the region of interest, which can be moved to a different arterial location if desired. It enables lower contrast use and reduces scan-to-scan and patient-to-patient variability in arterial opacification.
Test Bolus
Another method to optimize arterial contrast opacification is that of a test bolus or timing bolus acquisition. Described by a number of authors,38,40 this technique involves intravenous administration of a small bolus (20 to 30 mL) of contrast material followed by serial CT data acquisitions at one table position, usually at the levels described for bolus tracking. Images are acquired, after a scan delay of 8 to 10 seconds, every 1 to 2 seconds for a predetermined number of images (20 to 40) or until the CT technologist chooses to manually stop the acquisition after the contrast peak within the aorta. A time versus Hounsfield unit (attenuation) curve is then generated by placing a region of interest over the contrast-opacified aorta. The time taken to reach peak opacification is then used as the scan delay for the actual CTA and thus corresponds to the time taken for the contrast material to pass from the intravenous injection site of interest. This method is useful as it detects variable transit times between patients with different hemodynamic states and allows individualization of scan delays.
Adaptive Method
The runoff vessels in the symptomatic limb can be problematic with CTA as a result of proximal/in-flow stenosis or, alternatively, distal hyperemia at the site of arterial ulceration; these can cause arterial flow discrepancy between the two lower limbs. Thus, one limb will have a faster flow rate than the other, resulting in good contrast opacification of the arteries ipsilaterally but failed opacification contralaterally. CT fails at eliciting dynamic information. This problem may be somewhat reduced by use of an adaptive method of contrast detection that was described by Qanadli and associates.41 This method is similar to that of a test bolus technique in that a small 30-mL contrast bolus is administered intravenously, followed by two low-dose (20 mA, 120 kV) CT acquisitions. The first is at the level of the descending thoracic aorta (at vertebra level T12) acquired 20 seconds after the start of intravenous administration of the contrast material for 10 seconds; the second level is the popliteal arteries below the knee acquired 30 seconds after the start of the intravenous bolus (i.e., after the aortic level is finished). Three time-density curves are created, one from the aortic level and one from each of the popliteal artery levels. The time to peak contrast enhancement is then determined for each level (aortic time = T1; popliteal time = T2). If the right and left popliteal times are different, the symptomatic leg or the longer time is taken to be T2. The aortopopliteal transit time (Tt) is determined from T2 − T1. The CT gantry rotation time and table speed are then set to match Tt in order that the popliteal artery will be imaged at peak enhancement. T1 is the delay time between commencement of the usual intravenous contrast bolus and commencement of data acquisition.41 Laswed and colleagues42 applied this adaptive method clinically in patients with peripheral arterial disease, with DSA correlation, and determined that MDCTA has a sensitivity and specificity of 100% for arterial lesion detection on a per-patient basis. Analyzed on a per-segment basis, MDCTA had a sensitivity and specificity for lesion detection of 91% and 96%, respectively, in the below-knee arteries and 100% and 90%, respectively, in the distal pedal arteries. This method was found to be reproducible, had high image quality, avoided the problem of venous overlay, and resolved the issue of differential peripheral arterial opacification.42
Contrast Media Concentration
A recent review attempted to determine the difference that contrast media iodine concentration makes to image quality of MDCTA in the peripheral vasculature.43 All of the studies reviewed used iodine concentrations of 300 mg/mL and higher; whereas improved arterial enhancement and visualization were demonstrated with higher iodine concentrations, there was no clear evidence of a significant difference in diagnostic efficacy for the different iodine concentrations.43 Iezzi and coworkers,44 comparing iodine concentrations of 300 mg/mL with 400 mg/mL on a 4-detector scanner, also determined no significant differences in diagnostic ability of CTA for peripheral arterial disease. This could perhaps be explained by applying findings from the coronary CTA literature, whereby Becker and colleagues45 determined that coronary artery attenuation levels of 250 to 300 HU were optimal for the evaluation of coronary artery disease because higher attenuation values may underestimate the amount of atherosclerosis owing to obscuration of vessel wall calcification. In our institution, we use a contrast media iodine concentration of 350 mg/mL.
Dual-Head Power Injectors
To achieve the desired arterial Hounsfield unit, a fast iodinated contrast injection with a tight arterial contrast bolus is necessary. Thus, patients will need to have a well-positioned, large-bore (18-gauge), intravenous cannula within the antecubital fossa. A dual-head power injector permits both contrast material and saline to be administered separately, concurrently, and sequentially. This means that two separate injection phases are possible, the first with 100% iodinated contrast material and the second with a 100% saline flush. The advantages of this method are that the arterial contrast enhancement is improved and prolonged, the contrast dose is reduced because most of the administered contrast material is within the arterial side, and the saline flush at the end clears dense contrast material from the superior vena cava to avoid streak artifact.14,30,46 The value of a triphasic injection strategy with an extra second phase comprising a contrast-saline mixture could also potentially reduce the requirements for contrast material. The new multislice scanners in combination with dual-head injectors allow marked decrease in the amount of contrast material used for routine CTA. However, the total volume of contrast material administered for a routine abdominal CT study (usually 150 mL of 300 mg/mL concentration of contrast material) should not change if solid organs, such as liver, are evaluated in conjunction with CTA. Lowering of the total volume of contrast material may potentially reduce the sensitivity of lesion detection.12,32
Many authors have reported the use of gadolinium chelates for CTA in patients who have diminished renal function.47–50 Although gadolinium is radiodense and may be used as a contrast agent with radiography, many gadolinium-based products have higher osmolality than iodine-based contrast media and are therefore potentially more nephrotoxic. More important, there have been several reports of nephrogenic systemic fibrosis leading to serious physical disability in patients with end-stage renal disease receiving gadolinium-containing contrast agents.51,52
TECHNIQUES
Indications and Technique Description
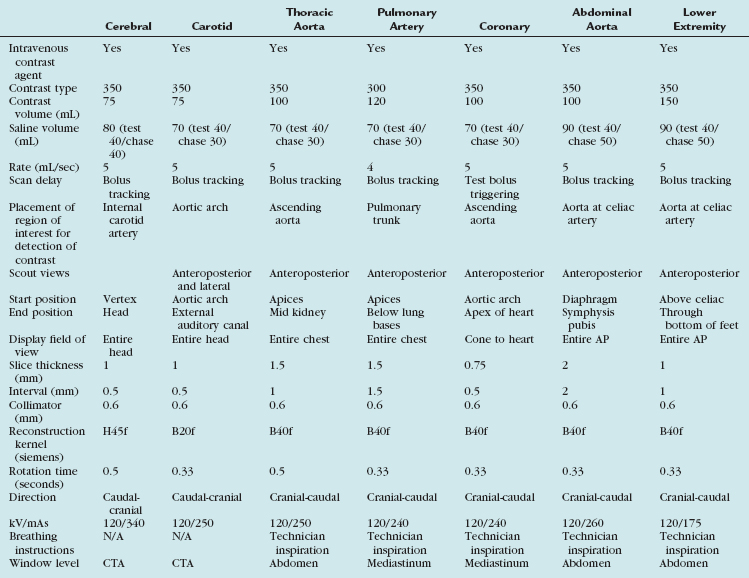
Scan protocols are highly variable and depend to a large extent on the type of MDCT scanner available (i.e., 4-, 16-, 64-, 128-, or 320-detector or dual energy) and also the manufacturer of the scanner. A suitable protocol should be chosen and programmed into the individual scanner for routine use. For the best CTA, a 16-slice scanner or higher should be used. A summary of the various protocols for the different vascular territories is outlined for a typical 64-slice MDCT scanner (Table 80-1).
TABLE 80-1 Summary of the Various Protocol Parameters for the Different Vascular Territories on a Typical 64-Slice MDCT Scanner
Cerebral CTA
Automated bolus tracking is the preferred technique to reliably obtain the optimal arterial phase by placing a region of interest on the internal carotid artery close to the skull base. An injection volume of 75 mL of a contrast agent with high iodine concentration (350 mg/mL) at a flow rate of 5 mL/sec is typically used. Images are acquired in the caudal to cranial direction with a slice thickness of 1 mm, slice interval of 0.5 mm, and 0.6 mm of collimation (Fig. 80-1).
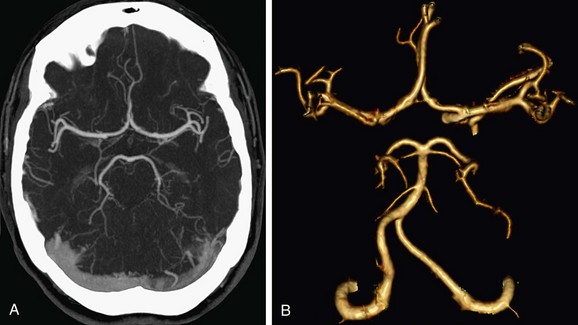
 FIGURE 80-1
FIGURE 80-1Carotid CTA
In the United States, stroke is the leading cause of adult disability and the third leading cause of death; only heart disease and cancer cause more deaths annually. About 80% of strokes are ischemic strokes. Ischemic cerebrovascular events are often related to atherosclerotic narrowing at the carotid bifurcation. Conventional DSA is the reference standard for the evaluation of carotid artery disease.53,54 The advantage of noninvasive CTA is the reduction in cost and procedural risks. With conventional DSA, several studies have demonstrated up to a 4% risk of transient ischemic attack or minor stroke, a 1% risk of major stroke, and a small (<1%) risk of death.55 Plaque composition can be evaluated by CTA, which is an important indicator of plaque stability and helps with the assessment of risk factors for thromboembolic events. Noninvasive CTA provides the necessary information required before carotid endarterectomy and endovascular therapies.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


