CHAPTER 44 Congenital Cholesteatoma of the Petrous Apex
Epidemiology
The petrous apex has the shape of a three-sided pyramid. The base of this pyramid is formed from anterior to posterior by the carotid canal, the cochlea, the vestibule, and the semicircular canals. The internal auditory meatus divides this region into an anterior subdivision and a posterior subdivision, also known as the meato-labyrinthine area located between the meatus and the semicircular canals. However, only those cholesteatomas that involve the anterior subdivision are considered as true petrous apex cholesteatomas.
Congenital cholesteatoma of the petrous apex, also known as primary petrosal cholesteatoma, is believed to arise from persistent embryonic cell rests of epidermal tissue within the petrous bone. This is believed to happen during cephalic flexure of the embryonic head, when the mesenchyme that eventually forms the petrous temporal bone traps the epithelial cells from epithelial invagination, called a Seessel pocket between the third and fifth week of fetal life. This can lead to accumulation of epithelial cells and keratin.
Clinical Features
Congenital cholesteatomas of the petrous apex may occur without otorrhea and in an otherwise normal temporal bone. Headache is the commonest symptom. The apical cholesteatoma can extend toward the horizontal portion of the internal carotid artery, the trigeminal nerve, or the dura of the middle or posterior cranial fossa. The commonest presenting symptom is unilateral hearing loss, followed by palsies of cranial nerve VII. They can also present with vertigo or, rarely, with trigeminal symptoms.
Pathology
Congenital cholesteatoma is a solid lesion, lined with stratified squamous epithelium and filled with debris of pearly white whirls of keratin and cholesterol crystals that originate from progressive desquamation of the epithelium.
Treatment
Surgical excision is the treatment of choice. The translabyrinthine-transcochlear (transotic) approach, infralabyrinthine approach, and infracochlear approach represent the most direct surgical approaches. As opposed to surgical treatments for cholesterol granulomas and arachnoid cysts, these are aggressive approaches that require sacrifice of any residual hearing with or without transposition of the facial nerve.
The middle cranial fossa approach, which may allow for hearing preservation, may be performed in patients with good hearing and normal facial nerve function, but requires a craniotomy, affords poor access, and may involve traction on important neurologic structures with potential for injury.
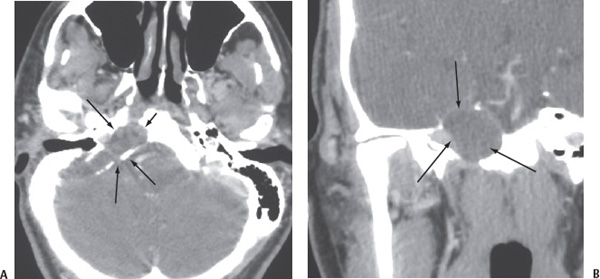
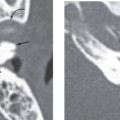
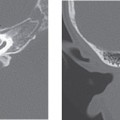
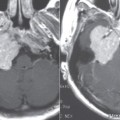
Figure 44-1
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


