Homogeneous opacity obscuring vessels
Air bronchograms
Ill-defined or fluffy opacities
“Air alveolograms”
Patchy opacities
“Acinar” or air-space nodules
Preserved lung volume
Extension to the pleural surface
“CT angiogram” sign
5 to 10 mm in diameter, that occur due to focal consolidation (Fig. 2-5). Although these nodules approximate the size of acini, they tend to be centrilobular and peribronchiolar rather than acinar. They may be seen as the only finding of consolidation or may be seen in association with larger areas of consolidation, usually at the edges of the more abnormal lung.
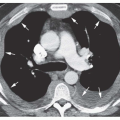
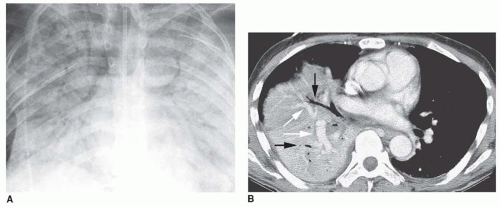 FIG. 2.1. Consolidation: homogeneous opacity obscuring vessels, air bronchograms, and the CT angiogram sign. A: Right lung consolidation due to pulmonary edema. Air bronchograms are visible bilaterally within the consolidated lung and pulmonary vessels are obscured. B: Enhanced CT in a patient with right middle and lower lobe pneumonia shows homogeneous consolidation, preserved lung volume, air bronchograms (black arrows), and opacified vessels (white arrows), appearing denser than surrounding consolidated lung (i.e., the “CT angiogram” sign). |
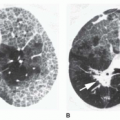
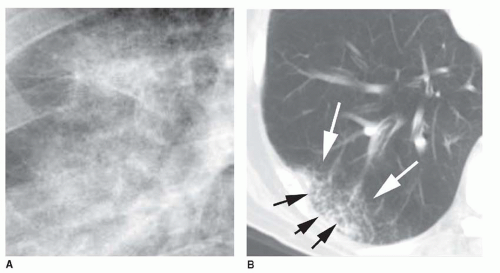 FIG. 2.2. Consolidation: ill-defined, fluffy opacities with “air alveolograms.” A: Detailed view of incomplete right lower lobe consolidation shows fluffy, ill-defined opacity containing small rounded lucencies. These lucencies have been termed air alveolograms, although they do not correspond to alveoli. B: Ill-defined fluffy consolidation (white arrows) is visible on CT in a patient with right lower lobe pneumonia. Small focal lucencies (black arrows) within the area of consolidation are “air alveolograms.” |
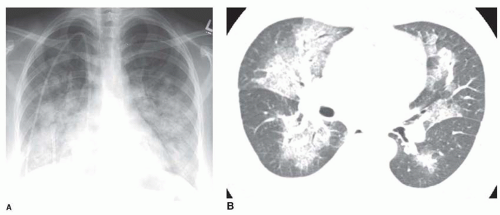 FIG. 2.3. Consolidation: patchy opacities. A: Chest radiograph in a patient with pulmonary edema due to renal failure shows patchy perihilar consolidation. B: Patchy areas of fluffy consolidation are seen on CT. The fluffy margins are due to variable involvement of alveoli at the edges of the pathologic process. |
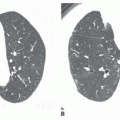
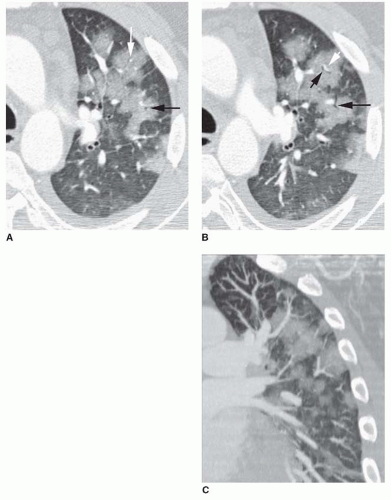 FIG. 2.4. Consolidation: patchy opacities with lobular consolidation. A, B: Contrast-enhanced HRCT in a patient with bronchopneumonia and lobular consolidation. Individual lobules are consolidated while others appear normal. Centrilobular arteries (white arrow) and bronchi (black arrows) are visible within consolidated lobules. C: Coronal reconstruction also shows the lobular distribution of the patchy lung opacities. |
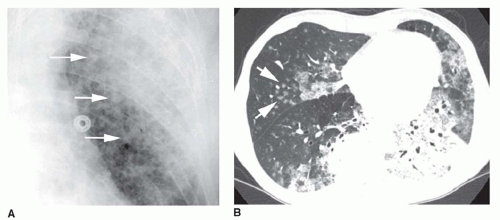 FIG. 2.5. Consolidation: acinar or air-space nodules. A: Chest radiograph shows a patchy left upper lobe pneumonia. Ill-defined nodular opacities less than 1 cm in diameter (arrows) are visible on the edge of the area of denser consolidation. These represent air-space or acinar nodules. B: CT (5-mm slice thickness) in a patient with bilateral consolidation. Air bronchograms are visible in the left lower lobe. Patchy consolidation and ground-glass opacities are present. Air-space nodules are visible in the right middle lobe (arrows) and the right lower lobe. These nodules are ill-defined, 5 to 10 mm in diameter, and centrilobular in distribution. |
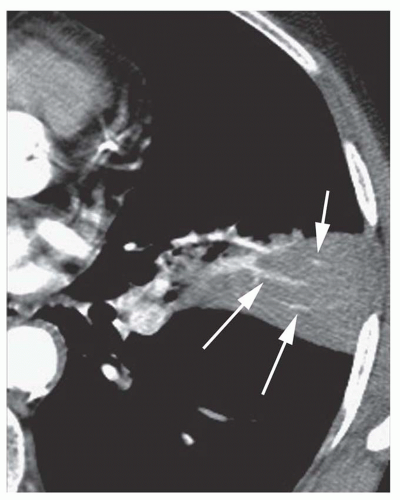 FIG. 2.6. Consolidation: the CT angiogram sign. Contrast-enhanced CT in a patient with pneumonia shows focal consolidation. Opacified arteries (arrows) appear denser than consolidated lung (i.e., the CT angiogram sign). The consolidation borders on the major fissure posteriorly and appears segmental. |
Water (e.g., the various types of pulmonary edema)
Blood (e.g., pulmonary hemorrhage)
Pus (e.g., pneumonia)
Cells (e.g., bronchioloalveolar carcinoma, lymphoma, eosinophilic pneumonia, organizing pneumonia [bronchiolitis obliterans organizing pneumonia or BOOP], hypersensitivity pneumonitis)
TABLE 2.1 Differential Diagnosis of Diffuse Consolidation
Water (edema) (see Chapter 11)
Hydrostatic (cardiogenic) pulmonary edema
Heart failure
Left atrial or pulmonary venous obstruction
Volume overload
Low intravascular oncotic pressure
Hypoalbuminemia
Liver disease
Renal failure
Increased permeability (noncardiogenic) pulmonary edema
With diffuse alveolar damage (acute respiratory distress syndrome [ARDS])
Acute interstitial pneumonia
Aspiration of gastric acid
Drugs
Fat embolism
Infection and sepsis
Near-drowning
Pneumonia
Radiation
Shock
Toxic fumes or gases
Trauma
Without diffuse alveolar damage
Any cause of ARDS, in a mild form
Drug reactions
Hantavirus pulmonary syndrome
Transfusion reaction
Mixed types of edema
Air embolism
High-altitude pulmonary edema
Neurogenic pulmonary edema
Posttransplantation edema
Postpneumonectomy
Reexpansion edema
Reperfusion edema
Tocolytic therapy
Hydrostatic and permeability edema
Blood (hemorrhage) (see Chapter 19)
Aspiration of blood
Bleeding diathesis
Anticoagulation
Chemotherapy
Leukemia
Low platelets
Collagen-vascular disease and immune complex vasculitis
Systemic lupus erythematosus most common
Behçet’s syndrome
Henoch-Schönlein purpura
Antiphospholipid syndrome
Goodpasture’s syndrome
Idiopathic pulmonary hemosiderosis
Trauma
Vasculitis
Wegener’s granulomatosis
Churg-Strauss granulomatosis
Microscopic polyangiitis
Pus (pneumonia)
Bacterial pneumonia
Pneumonia in an immunosuppressed patient
Tuberculosis
Nontuberculous mycobacteria
Fungal pneumonia (histoplasmosis, aspergillosis most common)
Atypical organisms
Virus
Pneumocystis
Cells
Neoplasm
Bronchioloalveolar carcinoma
Lymphoma and other lymphoproliferative diseases
Eosinophilic pneumonia or other eosinophilic diseases
Organizing pneumonia (BOOP)
Hypersensitivity pneumonitis
Idiopathic interstitial pneumonias
Nonspecific interstitial pneumonia
Desquamative interstitial pneumonia
Sarcoidosis
Other substances
Alveolar proteinosis (lipoprotein)
Lipoid pneumonia (lipid)
Other substances (e.g., lipoprotein in alveolar proteinosis, lipid in lipoid pneumonia).
Nonetheless, several patterns of diffuse consolidation may suggest possible causes.
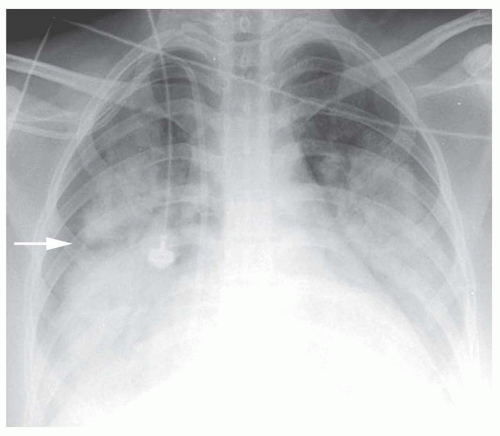 FIG. 2.7. Perihilar “bat-wing” consolidation in pulmonary edema. Chest radiograph in a patient with pulmonary edema due to renal failure (note the dialysis catheter in the right atrium) shows a distinct perihilar bat-wing pattern of consolidation. The lung periphery is spared. Note the lucency at the level of the minor fissure (arrow) because of sparing of peripheral lung adjacent to the fissure. |
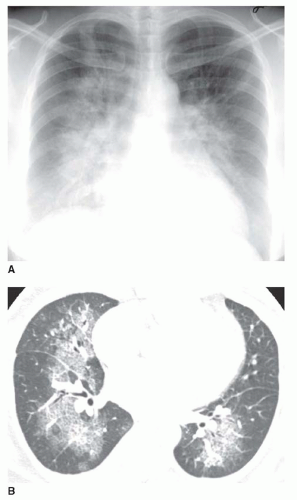 FIG. 2.8. Perihilar “bat-wing” consolidation in pulmonary edema. A: Chest radiograph shows a distinct perihilar predominance of consolidation. The heart is enlarged. B: CT shows sparing of the lung periphery. |
viral pneumonia (cytomegalovirus [CMV], measles), endobronchial spread of bronchioloalveolar carcinoma, pulmonary hemorrhage, or sometimes aspiration.
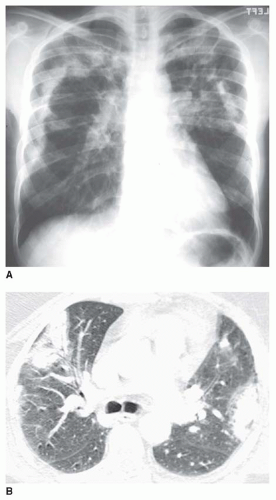 FIG. 2.9. Peripheral subpleural (reverse bat-wing) consolidation. A: Chest radiograph in a patient with chronic eosinophilic pneumonia shows areas of consolidation in the subpleural lung. The perihilar regions are spared. B: CT in a patient with BOOP shows patchy areas of consolidation in the subpleural lung. |
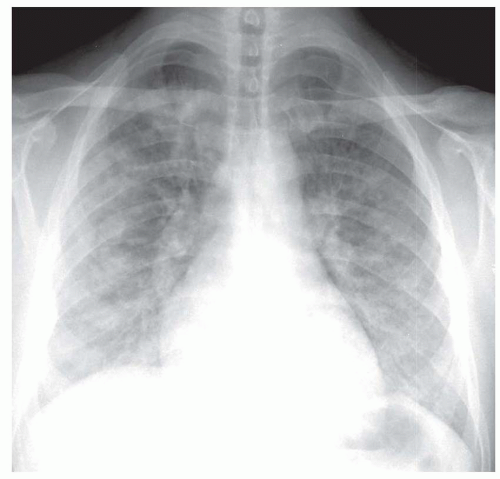 FIG. 2.10. Diffuse patchy consolidation in a patient with viral pneumonia. |
eosinophilic pneumonia; atelectasis; or rarely focal edema. The appearance of focal consolidation may also result from confluent interstitial disease, as in patients with sarcoidosis. The appearance or pattern of focal or multifocal consolidation may be helpful in differential diagnosis.
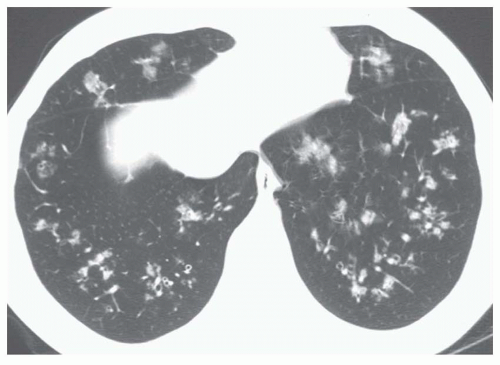 FIG. 2.11. Diffuse air-space nodules in bronchopneumonia. Multiple small nodular opacities are typical of spread of infection through the airways. This represented a bacterial bronchopneumonia, but other organisms such as TB, MAC, fungus, or viruses may be involved. |
TABLE 2.2 Differential Diagnosis of Focal Consolidation | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
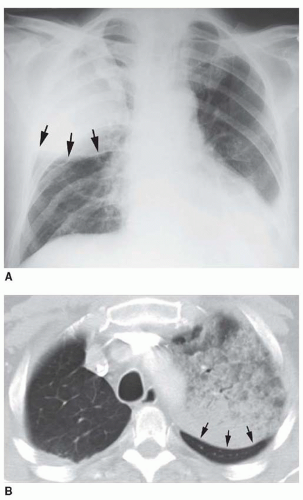 FIG. 2.12. Lobar consolidation with expansion. A: A patient with right upper lobe consolidation due to Klebsiella pneumonia shows downward bowing of the minor fissure (arrows) because of lobar expansion. B: Bronchioloalveolar carcinoma involving the left upper lobe with posterior bulging (arrows) of the left major fissure. |
myocardial infarction resulting in papillary muscle rupture and mitral valve prolapse; it occurs because a jet of regurgitant blood is directed into the right superior pulmonary vein. Focal pulmonary hemorrhage may lead to a lobar consolidation. Lobar consolidation is uncommon with pulmonary embolism.
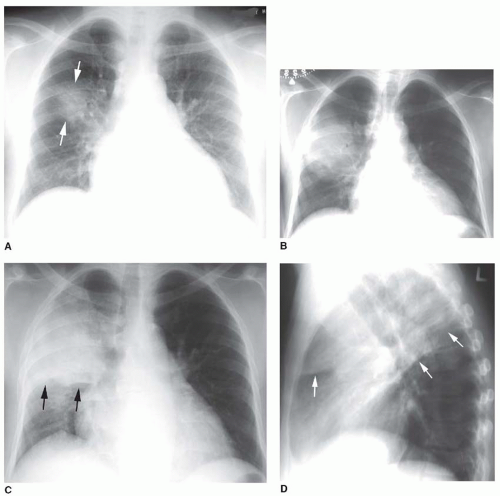 FIG. 2.13. Spherical consolidation due to pneumonia. A: On the initial radiograph, a patient with Legionella pneumonia shows a poorly defined area of consolidation (arrows) in the right upper lobe. This may be termed “round pneumonia.” B: Over the next several days, the spherical consolidation increases in size because of local interalveolar spread. This appearance may be seen in the early stages of lobar pneumonias. C: Further progression results in consolidation of the right upper lobe, marginated by the minor fissure (arrows). D: A lateral view at the same time as C shows upper lobe consolidation marginated by the major and minor fissures (arrows). Partial right middle lobe consolidation is also present. |
sphere of consolidation as more and more alveoli become involved. As the growing sphere reaches a pleural surface or fissure and cannot spread further, it becomes lobar.
 FIG. 2.14. Segmental consolidation. A patient with pneumonia shows consolidation of the lateral segment of the right middle lobe. The segmental bronchus is seen within the consolidated lung as an air bronchogram. The medial segment, adjacent to the right heart border, is normally aerated. The consolidated segment borders posteriorly on the major fissure. |
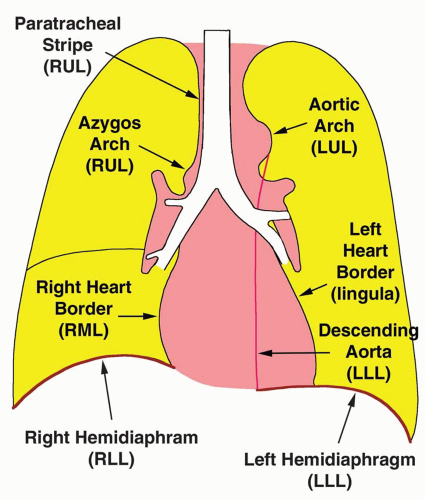 FIG. 2.15. Anatomic relationships used with the silhouette sign. Obscuration of the borders shown in this diagram are associated with consolidation of the listed lobes. RUL, right upper lobe; RML, right middle lobe; RLL, right lower lobe; LUL, left upper lobe; LLL, left lower lobe. |
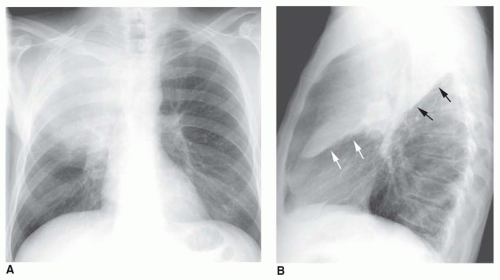 FIG. 2.16. The silhouette sign in right upper lobe pneumonia. A: Consolidation of the right upper lobe obscures (i.e., silhouettes) the border of the right superior mediastinum and superior vena cava. The upper part of the right hilum is also invisible. B: On the lateral view, the consolidated upper lobe is outlined superiorly by the upper aspect of the major fissure (black arrows). Inferiorly, it is outlined by the minor fissure (white arrows). (Figure continues.) |
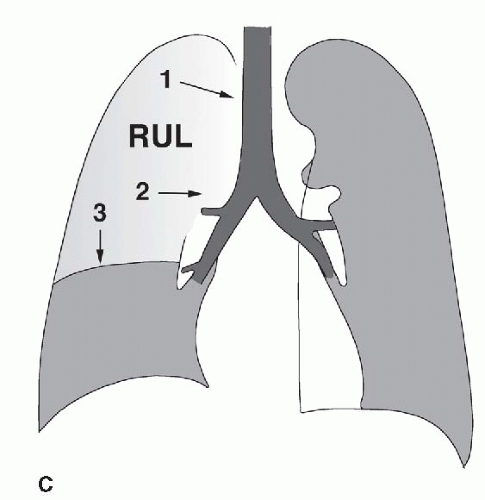 FIG. 2.16. (Continued.) C: Typical findings of right upper lobe consolidation: (1) obscuration of the right superior mediastinum, (2) obscuration of the superior right hilum, and (3) opacity marginated inferiorly by the minor fissure.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|