(see Fig. 22-5). Attachment to the tracheal wall may be either broad based (Fig. 22-5) or narrow and pedunculated. CT may underestimate the longitudinal extent of the tumor; submucosal spread may be difficult to see on CT. However, CT is superior to bronchoscopy in evaluating extraluminal spread and the trachea distal to an obstructing lesion.
 FIG. 22.1. The normal trachea. A: HRCT through the normal trachea. The tracheal wall (arrow) is outlined by mediastinal fat externally and usually is visible as a 1- to 2-mm soft-tissue stripe. The posterior tracheal membrane usually appears thinner than the anterior and lateral tracheal walls, and is variable in shape due to its lack of cartilage. At this level, it is partially obscured by the esophagus. B: At the level of the aortic arch, the tracheal wall (arrows) is outlined by mediastinal fat and the right lung in the region of the right paratracheal stripe. The tracheal wall appears thin. C: Diagrammatic representation of the normal components of the tracheal wall. |
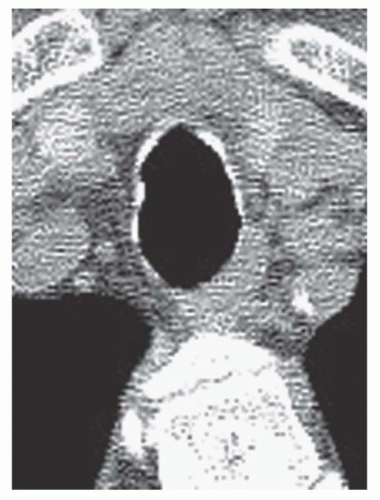 FIG. 22.2. Normal calcification of tracheal cartilage in an elderly woman. Discontinuous calcification of the tracheal wall reflects calcification of individual cartilage rings. The tracheal wall appears thin. |
 FIG. 22.3. Normal expiratory CT. A: On inspiration, the trachea has a rounded appearance. B: During a dynamic forced expiratory scan, there is marked anterior bowing of the posterior tracheal membrane (arrow). This appearance is normal. Little side-to-side narrowing occurs because of the tracheal cartilage. |
TABLE 22.1 Tracheal Tumors | ||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||
 FIG. 22.4. Adenoid cystic carcinoma of the proximal trachea. An eccentric narrowing (arrows) of the tracheal lumen is caused by a sessile mass arising from the right tracheal wall. |
 FIG. 22.5. Adenoid cystic carcinoma of the trachea. A: A large mass (large arrows) in the upper trachea markedly narrows the tracheal lumen (small arrow) and invades the mediastinum. B: On a sagittal reconstruction, the mass (arrows) can be seen to arise from the posterior tracheal wall. This location is typical of adenoid cystic carcinoma. |
 FIG. 22.6. CT appearances of primary tracheal tumor. A: Tracheal malignancies may appear polypoid, sessile, or circumferential. B: Adenoid cystic carcinoma results in a sessile mass (M) arising from the posterior tracheal wall and protruding into the tracheal lumen. The mass extends into the adjacent mediastinum (arrows). |
 FIG. 22.7. Esophageal carcinoma with tracheal invasion. Tumor has invaded the trachea and is seen as soft tissue (small arrows) internal to the calcified tracheal cartilage (large arrows). The tracheal lumen is narrowed. |
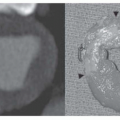
 FIG. 22.8. Tracheal metastasis. Tracheal metastases may result in tracheal compression with inward displacement of the tracheal wall, an endotracheal mass, or a combination of these findings. A, B: There is narrowing of the trachea with an endoluminal mass (arrow). C: Soft-tissue window at the same level as (B) shows a mass involving the right tracheal wall and mediastinal soft tissues (arrows). |
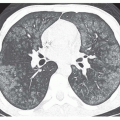
 FIG. 22.9. Tracheobronchial papillomatosis with tracheal wall thickening. A: Concentric thickening of the tracheal wall (arrows) is due to diffuse involvement by papillomas. The tracheal lumen is markedly narrowed. B: Multiple cystic pulmonary lesions may be seen in some patients with tracheobronchial papillomatosis. |
with saber-sheath trachea, relapsing polychondritis, or tracheobronchomegaly. It may be localized, or it may involve a long tracheal segment.
TABLE 22.2 Non-Neoplastic Tracheal Diseases | ||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


