Chapter 9 Contraction assessment
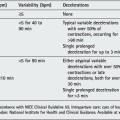
Effective contractions (the powers) of the uterus are an essential prerequisite for labour and vaginal delivery. The progress of labour, evidenced by dilatation of the uterine cervix and descent of the presenting part, is the final measure of contractions. During the journey through the birth canal (the passages), the passenger is intermittently squeezed and stressed by the contractions. Maternal blood flow into the uteroplacental space ceases when the intrauterine pressure (IUP) exceeds the pressure of flow of blood into the retroplacental area, which could be 30–45 mmHg. A well-grown fetus with good placental reserve tolerates this as ‘normal stress’ and displays no change in the fetal heart rate (FHR). A compromised fetus may show changes with this stress, and reduction of the retroplacental pool of blood due to contractions will be manifested as late decelerations. In a normal fetus, stress can be brought about by cord compression which will be shown as variable decelerations. The presence of atypical variable decelerations indicates that there is cord compression and at the same time there is reduction of retroplacental pool of blood (e.g. atypical variable decelerations with late recovery or a combination of variable and late decelerations). Oxytocin or prostaglandins are given expressly to increase the contractions; when they are given to induce labour the fetus is often already at risk. Particular care should be taken to ‘manage’ the contractions under these circumstances and to monitor the FHR continuously.
RECORDING
The commonest method of assessing contractions is with the hand placed on the abdominal wall over the anterior part of the uterine fundus. This permits observation of the duration and frequency of contractions. A subjective impression is gained of their strength. This is entirely adequate if performed intermittently in normal low-risk labour.
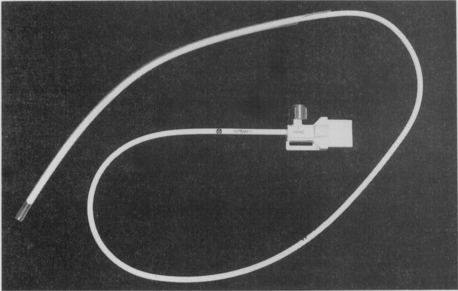
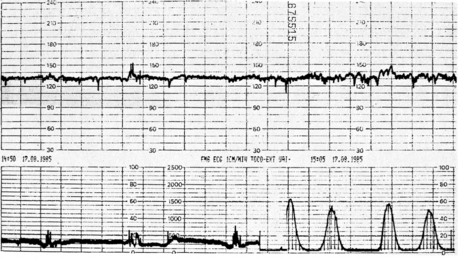
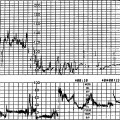
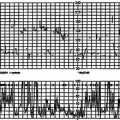
Continuous monitoring of uterine contractions is performed using external tocography. The tocograph transducer (Fig. 9.1) is a strain gauge device detecting forward movement and change in the abdominal wall contour due to change in shape of the uterus with an anterior thrust on account of the contraction; recording continuously what the hand feels intermittently. The transducer is placed without the application of jelly on the anterior abdominal wall, near the uterine fundus, and secured with an elastic belt. It is important to adjust the tension of the belt for comfort and to secure an adequate recording. Obesity and a restless mother can compromise this. In these circumstances, and in other clinical situations, there may be a role for palpation of uterine contractions or IUP measurement using an intrauterine catheter (Fig. 9.2). IUP measurement is the most effective method of recording contractions including a fairly precise measure of the strength in millimetres of mercury or kilopascals.87 The technology for this has been developed and several disposable, solid-state devices are available: the Intran II catheter (Fig. 9.3) (Utah Medical Products, Utah). Figure 9.4 shows the change in recording in an obese mother seen after converting from external to internal tocography over a period of 20 min.


MEASUREMENT
What are normal contractions? The most relevant measure of contractions in labour is their outcome: dilatation of the cervix and descent of the presenting part resulting in spontaneous vaginal delivery. The quality of contractions present is very variable. A simple assessment of the frequency of contractions (number per 10 min), the mean duration (in seconds) and a subjective impression of strength (weak, moderate or strong) usually suffices. The method of recording this is seen on the partogram (see Fig. 2.3). When IUP monitoring is being used the opportunity arises for greater precision. In 1957 Caldeyro-Barcia suggested Montevideo units using average pressure multiplied by frequency.88
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


