Fig. 4.1
(a) Axial T2-weighted spin echo image (TE: 116/TR: 6450) showing no suspicious low signal intensity area in the peripheral zone in a 63-year-old man with PSA level at 7.2 and history of two negative sets of biopsy. (b) Dynamic axial T1-weighted gradient echo sequences (TE: 1.46/TR: 3.77/10°) with fat suppression show an early enhancement, whereas the surrounding PZ shows no enhancement (white arrow). (c) Axial TRUS after contrast injection shows the corresponding hypervascular area on the CPS-mode images (white arrow). Histopathologic examination revealed a prostate carcinoma Gleason 6 (3 + 3) on targeted biopsies only
4.3 CEUS Examination of the Prostate
While contrast-enhanced ultrasound is mainly used for perfusion measurement of the heart and for the detection of liver malignancies, CEUS into the prostate has been proposed because prostate cancer tissue is associated with an increased microvessel density due to the proliferation of neovessels. US contrast agents enable improved detection of low-volume blood flow by increasing the signal-to-noise ratio, while conventional color/power Doppler US imaging cannot visualize microvessels (Fig. 4.2). Therefore, contrast agents, such as Sonovue® (sulfur hexafluoride), Definity® (perflutren lipid microspheres), or Sonazoid® (perflubutane), allow real-time visualizing of the contrast enhancement of the whole prostate which differentiates between normal prostate, adenoma, and carcinoma.
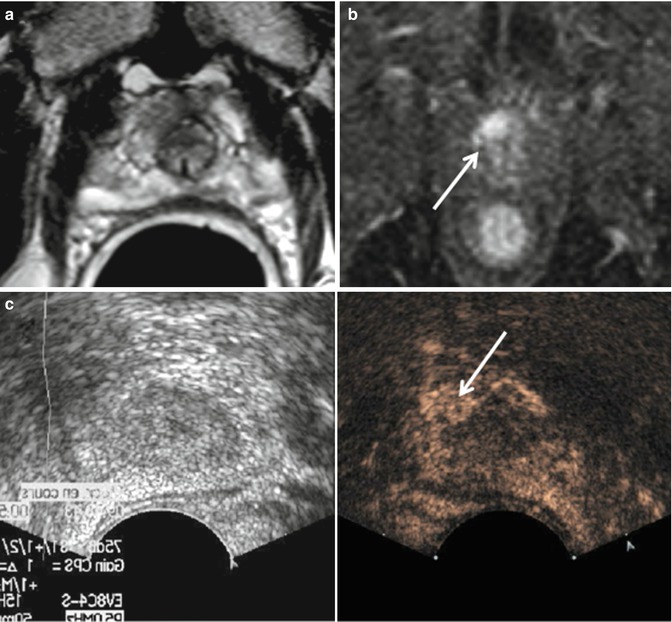
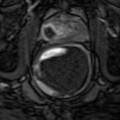
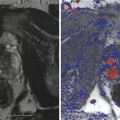
Fig. 4.2
(a) Axial T2-weighted spin echo image (TE: 116/TR: 6450) showing an anterior hypointense lesion suspicious for prostate cancer in a 68-year-old man with PSA level at 5.4 and history of 1 negative set of biopsy. (b) Dynamic axial T1-weighted gradient echo sequences (1.46/3.77/10°) with fat suppression show an early enhancement (white arrow), whereas the surrounding transition zone shows no enhancement. (c) Axial TRUS after contrast injection shows the corresponding hypervascular area on the CPS-mode images (white arrow). Pathological results concluded to a prostate carcinoma Gleason 7 (4 + 3) on targeted biopsies only
4.4 CEUS-Guided Biopsies
By improving sensitivity, CEUS has been shown to increase the detection of prostate cancer during the first set of biopsies. However, false-positive findings may result if the difference in specificity is not evident (Mitterbetger et al. 2010) due to flow abnormalities resulting from prostatitis or hyperplasia in the TZ. Several studies have been published on the topic and have confirmed the preliminary results of ultrasound-guided conventional gray-scale and/or color Doppler biopsies. These studies mainly compared contrast-enhanced US-targeted biopsy of the prostate with gray-scale US-guided systematic biopsy.
Ultrasound-guided color Doppler biopsies have been proposed. In the study of Frauscher et al. (2002), 230 patients were biopsied and cancer was found in 30 % patients (69/230), including 24.4 % (56/230) by contrast-enhanced targeted biopsy and in 22.6 % (52/230) by systematic biopsy. The detection rate for targeted biopsy cores (10.4 %) was significantly better than for systematic biopsy cores (5.3 %, P < 0.001), and contrast-enhanced targeted biopsy in a patient with cancer was 2.6-fold more likely to detect prostate cancer than systematic US-guided biopsy. Similar results were reported by Pelzer et al. (2005), who observed that a contrast-enhanced targeted biopsy was 3.1-fold more likely to detect cancer than systematic biopsy. However, the combined use of color Doppler-targeted and systematic biopsy allowed for maximal cancer detection with a detection rate of 37.6 % in patients with PSA 4–10 ng/ml. Based on Gleason score findings, Mitterberger et al. (2010) showed that contrast-enhanced biopsy detected significantly higher Gleason scores compared with systematic biopsy in a population of 690 patients. The Gleason score of all 180 cancers (26 %) detected by contrast-enhanced targeted biopsy was 6 or higher (mean 6.8) vs. a range from 4 to 8 (mean 5.4) for the 166 cancers (24 %) detected by systematic biopsy alone.
Based on a gray-scale harmonic CEUS evaluation, Matsumoto et al. (2010) compared radical prostatectomy specimens with the CEUS and were able to identify at least one tumor focus in 40 % of the cases (20/50 patients). When using CEUS alone, at least one tumor focus enhancement was seen in 62 % of the patients; when gray-scale and contrast-enhanced imaging were combined, identification of a tumor focus occurred in 80 % of the cases (40/50 patients). Moreover, Halpern et al. showed that cancer could be identified in 40 % of biopsies of 40 patients (Halpern et al. 2005). The same team confirmed this finding subsequently when authors compared contrast-enhanced harmonic imaging-targeted biopsies with systematic biopsies in 301 patients. In these studies, CEUS-guided biopsies were two times more likely to find cancer compared to systematic biopsy in patients with PCa. However, 20 % of cancers were missed with targeted biopsies and were detected on systematic biopsy alone. While the detection rate of carcinoma is higher with CEUS-guided biopsies, the authors concluded that systematic biopsies were still recommended. Sano et al. (2011) used harmonic imaging to perform 12-core systematic and targeted biopsies in 41 patients. In this study, significantly more cancers were found with CEUS-targeted biopsies compared with systematic biopsies (36.6 vs. 17.7 %).
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


