Key Points
- ▪
CCT angiography is the test of choice to define coronary artery aneurysms.
- ▪
The common occurrence of mural thrombosis of larger coronary artery aneurysms renders cardiac CT particularly able to determine the full size of the coronary artery aneurysm, beyond the means of conventional coronary angiography and beyond that of CMR.
Coronary aneurysms have been identified in 0.5% to 4% of patients undergoing coronary angiograms. The incidence among patients undergoing coronary CT angiography (CTA) has not been determined.
The most common definition of a coronary artery aneurysm is focal dilation of the artery, 1.5 times normal (adjacent reference segment or elsewhere maximal vessel) diameter, and limited to spherical or saccular dilation—a standard and borrowed convention of the definition of an aneurysm. Although generally small (just millimeters in diameter), coronary artery aneurysms may be extremely large. Aneurysms measuring 12 cm have been found.
Aneurysms are encountered most commonly in the right coronary artery but may be found in any coronary artery and may be multiple, especially in the setting of prior Kawasaki disease, where large aneurysms also are common. The left main stem coronary artery appears to be the least common site for coronary aneurysms, although this site is heavily represented in the literature.
Some reviews suggest male dominance of coronary aneurysms.
Formation of coronary aneurysm after percutaneous coronary intervention is relatively common in patients with Kawasaki disease, and the incidence varies from 15% to 18%.
Etiologies and Associations
- □
Half of all coronary artery aneurysms (50%) are associated with atherosclerotic coronary artery disease. Associated stenoses are common.
- □
Coronary artery disease (CAD)–associated
- •
Drug-eluting stents
- •
Cutting balloon
- •
Coronary ectasia
- •
Extensive coronary calcification
- •
Saphenous bypass grafts
- •
- □
Vasculitis
- •
Aortitis of all forms extending onto the proximal coronary arteries
- •
Polyarteritis nodosa (PAN)
- •
Kawasaki disease
- •
Hyperesoinophilic syndrome
- •
Other
- •
- □
Vascular disease–or syndrome-associated
- •
Fibromuscular dysplasia
- •
Supravalvular aortic stenosis
- •
- □
Marfan syndrome
- □
Infection (mycotic)
- □
Coronary artery arteriovenous fistulae
- □
Myocardial bridging
- □
Idiopathic
Risks
The risk from coronary artery aneurysms appears to be due mainly to the development of mural thrombus within the aneurysm sac and subsequent embolization of thrombus down the ongoing coronary artery or branch vessels. Because thromboembolism is the late outcome of large coronary aneurysms, the amount of embolized thrombus, and the ensuing coronary event, may be large.
- □
Acute coronary syndrome (ACS)
- □
Myocardial infarction not associated with stenosis in the same vessel
- □
Myocardial infarction and post-infarction tamponade
- □
Rupture and tamponade
- □
Myocardial infarction and right ventricular infarction/shock
- □
Cardiac arrest
- □
Sudden death
- □
Breakdown of the wall of the aneurysm with:
- •
Fistulization into an adjacent cavity
- •
Pericardial tamponade
- •
- □
Aneurysms also may compress adjacent structures:
- •
Chambers
- •
Superior vena cava (SVC): SVC syndrome
- •
Pulmonary artery
- •
- □
Aortic insufficiency
- □
Vasospasm elsewhere
- □
Thrombosis of a bare-metal stent inserted into an unappreciated aneurysm with extensive mural thrombus, which may dissolve and result in stent dislodgement
Treatment
- □
Prevention: Established for Kawasaki disease using intravenous gamma globulin and aspirin
- □
Observation
- □
Active treatment
- •
Anti-platelet and anticoagulation
- •
Percutaneous covered stent closure
- •
Percutaneous coil embolization (saphenous graft aneurysm)
- •
Surgical repair
- •
Ligation at the inflow and/or outflow and internal thoracic/mammary or saphenous bypass. Use of arterial conduits is anticipated to provide more lasting benefit to younger patients.
- •
Aneurysmectomy and end-to-end repair
- •
Resection with bypass
- •
Patch repair/reconstruction
- •
- •
Potential Coronary CTA Findings of Coronary Artery Aneurysms
- □
Aneurysmal dilation
- •
Solitary or multiple
- •
Spherical or saccular
- •
- □
Coronary ectasia
- □
Coronary stenoses
- □
Mural thrombus within the aneurysm
- □
Calcification of the aneurysm
- □
Fistulous drainage of the aneurysm
- □
Aneurysm located within a fistulous coronary anomaly
- □
Compression of adjacent chambers and structures
- □
Associated aneurysms of the aorta or other vessels
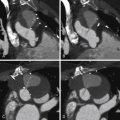
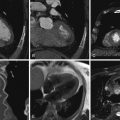
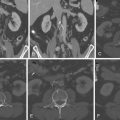
CCT Images of Coronary Artery Aneurysms
Examples are shown in Figures 11-1 through 11-15 and





Related posts:
 Overview of the Process, Exclusions and Risks, and Preparation
Overview of the Process, Exclusions and Risks, and Preparation
 CTA Assessment of Saphenous Vein Grafts and Internal Thoracic (Mammary) Arteries
CTA Assessment of Saphenous Vein Grafts and Internal Thoracic (Mammary) Arteries
 Coronary Ostial and Left Main Stem Lesions, Spasm, and Thrombus
Coronary Ostial and Left Main Stem Lesions, Spasm, and Thrombus
 Assessment of Left Ventricular Structural Abnormalities
Assessment of Left Ventricular Structural Abnormalities
 Cardiac and Paracardiac Masses
Cardiac and Paracardiac Masses
 Caval Anatomy: Variants and Lesions
Caval Anatomy: Variants and Lesions
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


