Graft
Preparation
Direction
LIMA
Pedicled
LAD/Dia/OM
Skeletonized
LAD/Dia/OM
Free graft
LAD/Dia/OM
RIMA
Pedicled
LAD/Dia/OM/proximal RCA
Skeletonized
LAD/Dia/OM/proximal RCA
Free graft
LAD/Dia/OM/proximal RCA
RA
Free graft
Any vessel
GEA
Skeletonized
PDA
Free graft
Distal LAD (prolonging LIMA)
GSV
Free graft
Any vessel
The left internal mammary artery is usually anastomosed to the left descending coronary artery, diagonals, and/or obtuse marginal branches both as a single graft (Fig. 12.1) or in a sequential arrangement. The right internal mammary artery is usually anastomosed to the left anterior descending coronary artery crossing the midline (Fig. 12.2A), to the proximal right coronary artery, to obtuse marginal branches or diagonals, via the transverse sinus (behind the aorta) (Fig. 12.2B), or to obtuse branches or diagonals (Fig. 12.3).
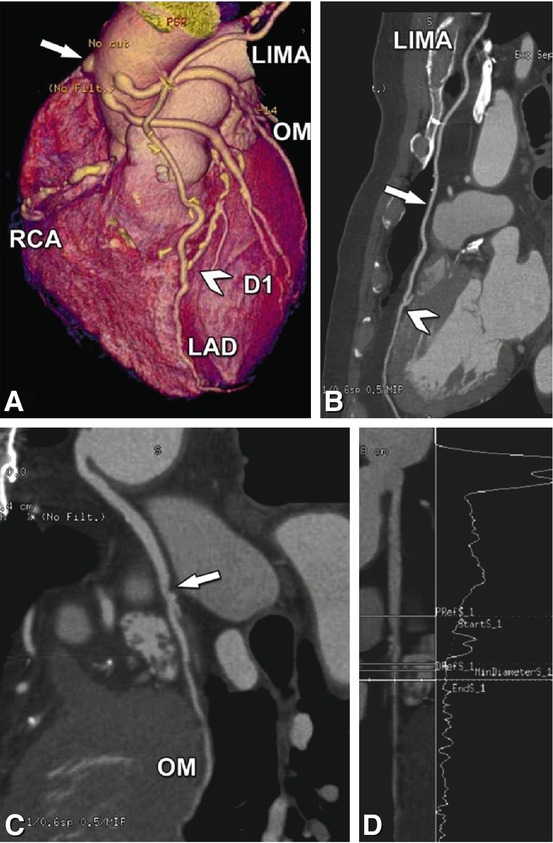
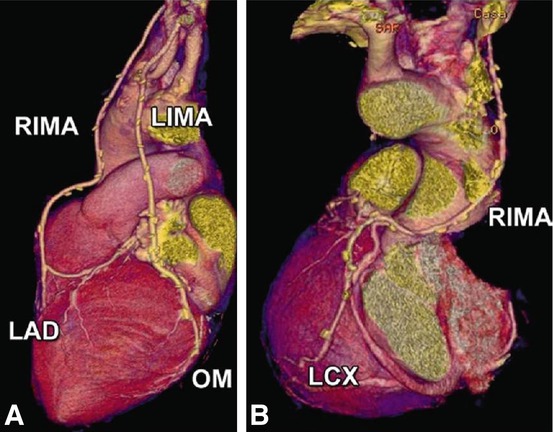
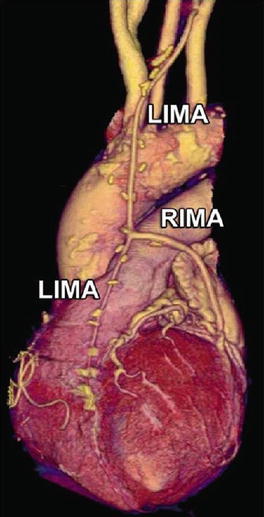
Fig. 12.1
64-year-old male patient who was underwent left internal mammary artery (LIMA, skeletonized) grafting to the left descending coronary artery and vein grafts to the right coronary artery (RCA), the diagonal branch (D1), and to the obtuse marginal branch (OM, Panel A, three-dimensional reconstruction) 14 years ago. CT was performed because of an inferior myocardial perfusion defect on single-photon emission computed tomography. The skeletonized LIMA graft is patent (arrow in Panel B, curved multiplanar reformation) with a normal distal anastomosis (arrowhead in Panels A and B) but the vein graft to the RCA is occluded (arrow in Panel A). The venous graft to the OM branch shows luminal narrowing (arrow in Panel C, curved multiplanar reformation), which was estimated to be not significant by quantitative analysis (14% diameter stenosis in Panel D, lumen stripe reformation)
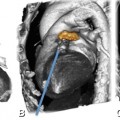
Fig. 12.2
Different examples of left and right internal mammary artery grafts. Panel A shows three-dimensional reconstructions of the CT in a 68-year-old female patient who underwent left internal mammary artery (LIMA, skeletonized) grafting to an obtuse marginal branch (OM) and right internal mammary artery (RIMA, also skeletonized) to the left anterior descending coronary artery (LAD) 6 years ago. The CT was performed because of atypical angina and shows that both arteries are patent (volume-rendered three-dimensional reconstruction). Panel B shows a RIMA (skeletonized) anastomosed to the left circumflex coronary artery (LCX) across the transverse sinus behind the aorta in a 58-year-old male patient who was operated on 8 years ago. CT was performed because of an inconclusive stress test. The grafts were patent in both patients
Fig. 12.3
66-year-old female who was operated on 7 years ago by left internal mammary artery (LIMA) to the left descending coronary artery, a right internal mammary artery (RIMA) used as free graft in Y configuration with the LIMA to revascularize an obtuse marginal branch. CT was carried out because of an inconclusive stress test. The grafts are patent without significant stenoses
The great saphenous vein is usually directly anastomosed to the aorta to revascularize any coronary artery both in a single graft (Figs. 12.4 and 12.5) or in a sequential arrangement (Fig. 12.6). The radial artery is also used as free graft to all coronary arteries as a single graft (Fig. 12.4C) or in sequential arrangement. It is more frequently attached in a Y-configuration to left or right internal mammary grafts and less commonly to the aorta. The gastroepiploic artery is only rarely used to revascularize the posterior descending coronary artery; sometimes it is used as a free graft to extend a left internal mammary graft anastomosed to the very distal part of left anterior descending coronary artery (Fig. 12.7).
Get Clinical Tree app for offline access
Fig. 12.4
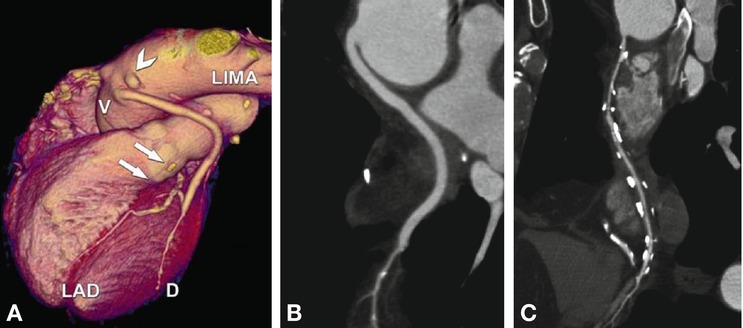
63-year-old male patient who was underwent left internal mammary artery (LIMA) to the left descending coronary artery (LAD), two single vein (V) grafts to the obtuse marginal branch and diagonal (D) branch (Panels A and B) as well as radial artery (free graft) to the descending posterior coronary artery (Panel C) 10 years ago. CT was performed because of a positive perfusion stress test (lateral wall). The venous graft to the marginal branch (arrowhead) and the LIMA (arrows) is occluded (Panel A, volume rendering) whereas the venous graft to the D branch is patent (Panel B




Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
