8 Cross-Sectional Computed Tomography and Magnetic Resonance Imaging Atlas of the Skull Base Optimal diagnostic evaluation and treatment planning for skull base pathology is contingent on accurate detection and determination of the anatomic extent of the lesion. Cross-sectional imaging techniques such as computed tomography (CT) and magnetic resonance imaging (MRI) enable detailed visualization of the intricate normal anatomy and disease spread at the skull base and play a central role in the diagnostic evaluation and surveillance of patients with skull base pathology. Skull base anatomy is complex consisting of different bones, soft tissues, and air-containing cavities. There are also complex anatomical relationships and potential pathways of disease spread. As a result, familiarity with the detailed anatomy of this area is a prerequisite for optimal diagnostic evaluation, and, frequently, a combination of different techniques such as CT and MRI is required for proper diagnosis and treatment planning. CT scans have a very high spatial resolution and can be acquired with short scan times. In addition to evaluation of soft tissues, CT enables excellent visualization of fine bone detail and anatomy. With modern high-resolution CT scans, the major skull base foramina and a wide array of anatomic structures and variations can be visualized with a high level of detail and confidence. CT is also the test of choice for visualization and determination of important anatomic variations in the paranasal sinuses that help guide endoscopic sinus surgery and help avoid complications. MRI examinations are longer to acquire than CT scans but have excellent soft-tissue contrast. These scans enable detailed evaluation of skull base anatomy and pathology, and in particular are excellent for characterization of soft-tissue abnormalities, intracranial spread of disease, and spread of disease across different spaces and along the major neural pathways. The purpose of this atlas is to provide an overview of the imaging anatomy of the skull base on CT and MRI. In preparing this atlas, our hope is to provide both basic and essential information for the less familiar reader as well as more detailed and intricate anatomical information for advanced interpretation in an easily accessible atlas format that can be used as an educational tool or as a reference in clinical practice. In this atlas, CT is mainly used for demonstration of detailed bone anatomy and related important anatomical relationships, whereas MRI is used to demonstrate the normal soft-tissue anatomy in adjacent structures and spaces such as the sella, cavernous sinus, major foramina, and posterior fossa. Axial high-resolution CT image(s) without contrast ( Axial high-resolution CT image(s) without contrast ( Axial high-resolution CT image(s) without contrast ( Axial high-resolution CT image(s) without contrast ( Fig. 8.2 Fig. 8.4 Fig. 8.6 Fig. 8.8 Fig. 8.10 Fig. 8.12 Fig. 8.14 Fig. 8.16 Axial high-resolution CT image(s) without contrast ( Axial high-resolution CT image(s) without contrast ( Axial high-resolution CT image(s) without contrast ( Fig. 8.19 Fig. 8.21 Fig. 8.23 Fig. 8.25 Fig. 8.27 Axial high-resolution CT image(s) without contrast ( Axial high-resolution CT image(s) without contrast ( Axial high-resolution CT image(s) without contrast ( Coronal reformats from high-resolution CT images without contrast ( Coronal reformats from high-resolution CT images without contrast (
8.1 Introduction
8.2 Atlas of Osseous Anatomy of the Skull Base
8.2.1 Axial Image Set
Axial Computed Tomography (No Contrast)
![]() Fig. 8.1,
Fig. 8.1, ![]() Fig. 8.2,
Fig. 8.2, ![]() Fig. 8.3,
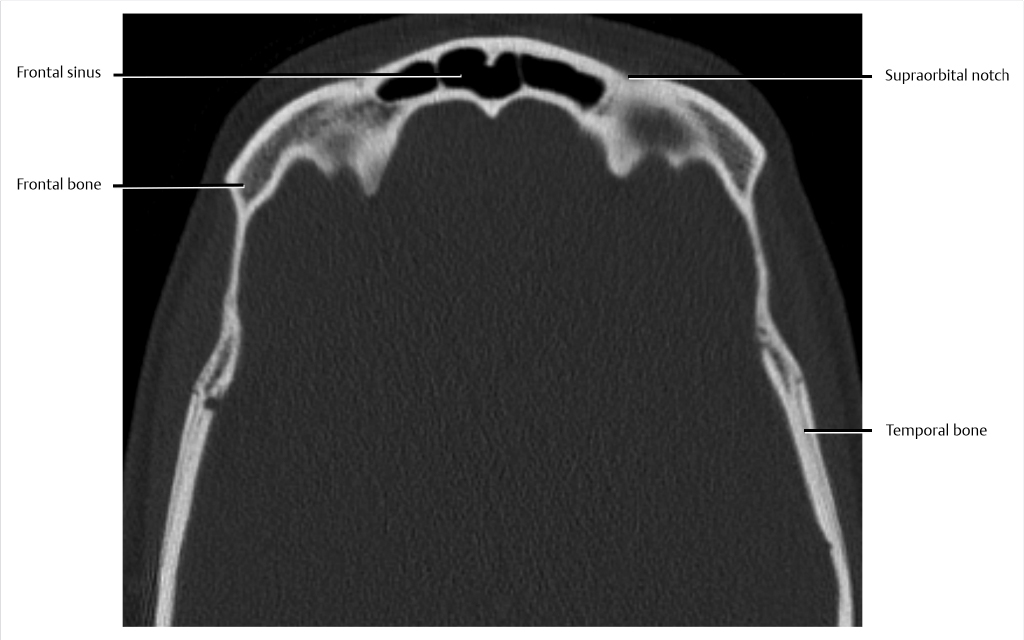
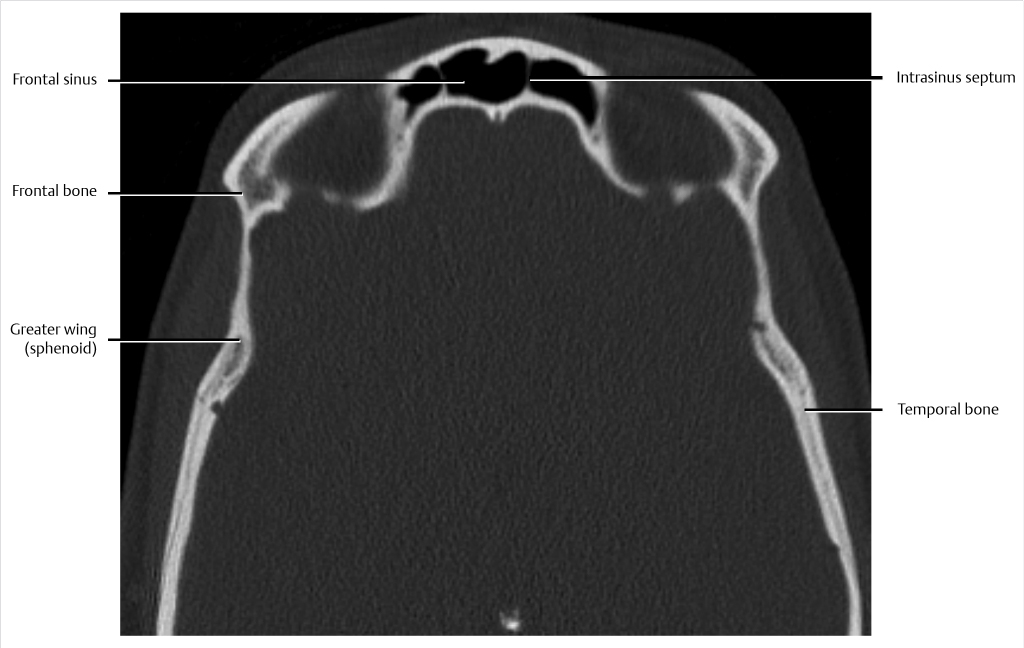
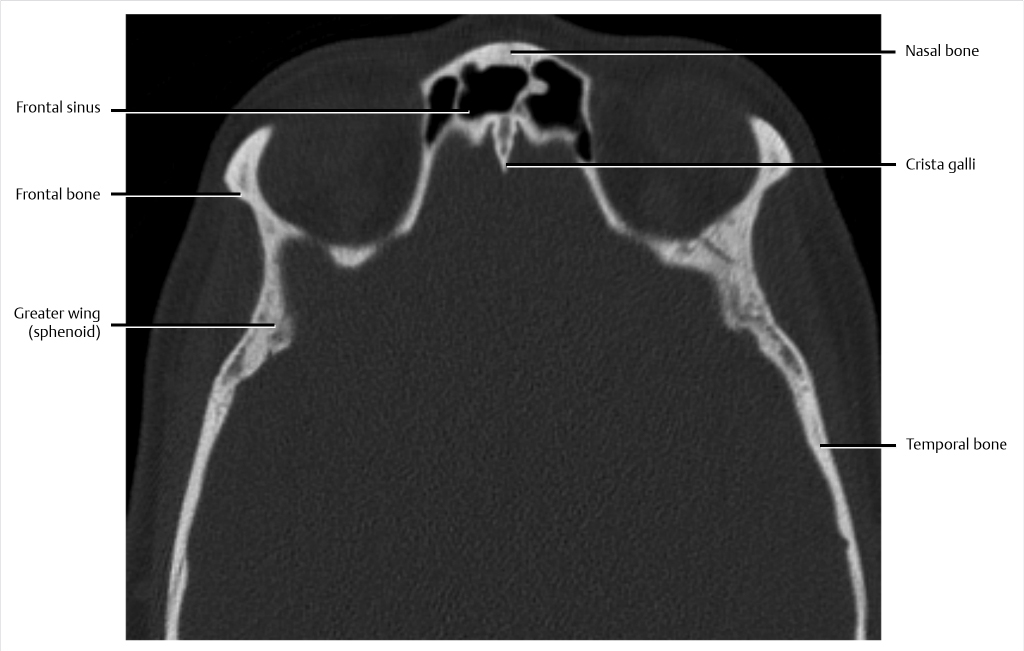
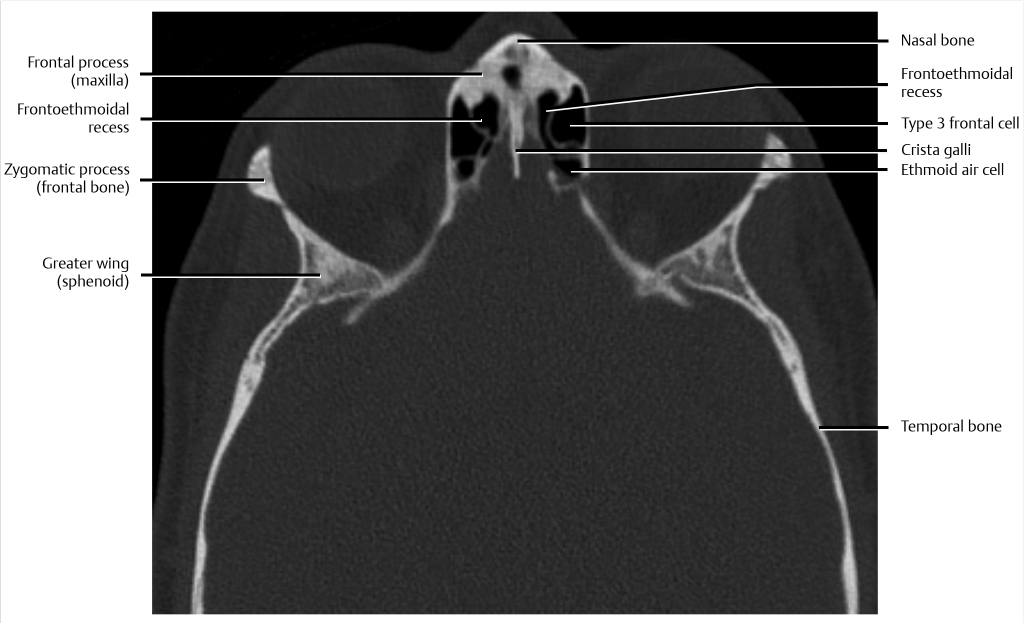
Fig. 8.3, ![]() Fig. 8.4). The skull base and paranasal sinuses are formed by the fusion of multiple bones, as shown. The anterior skull base can be broadly described as constituting the floor of the anterior cranial fossa and the roof of the nose, ethmoid air cells, and orbits. These anatomic relationships are important and constitute different potential pathways of spread of pathology. Some of the key anatomic structures are constant, but others, such as paranasal sinuses, can have significant variations in their detailed anatomy. In the case of frontal sinuses, there is typically an inter-sinus septum that may be midline or paramedian in location. In addition, there can be intra-sinus septa within the frontal sinuses.
Fig. 8.4). The skull base and paranasal sinuses are formed by the fusion of multiple bones, as shown. The anterior skull base can be broadly described as constituting the floor of the anterior cranial fossa and the roof of the nose, ethmoid air cells, and orbits. These anatomic relationships are important and constitute different potential pathways of spread of pathology. Some of the key anatomic structures are constant, but others, such as paranasal sinuses, can have significant variations in their detailed anatomy. In the case of frontal sinuses, there is typically an inter-sinus septum that may be midline or paramedian in location. In addition, there can be intra-sinus septa within the frontal sinuses.
![]() Fig. 8.5,
Fig. 8.5, ![]() Fig. 8.6,
Fig. 8.6, ![]() Fig. 8.7,
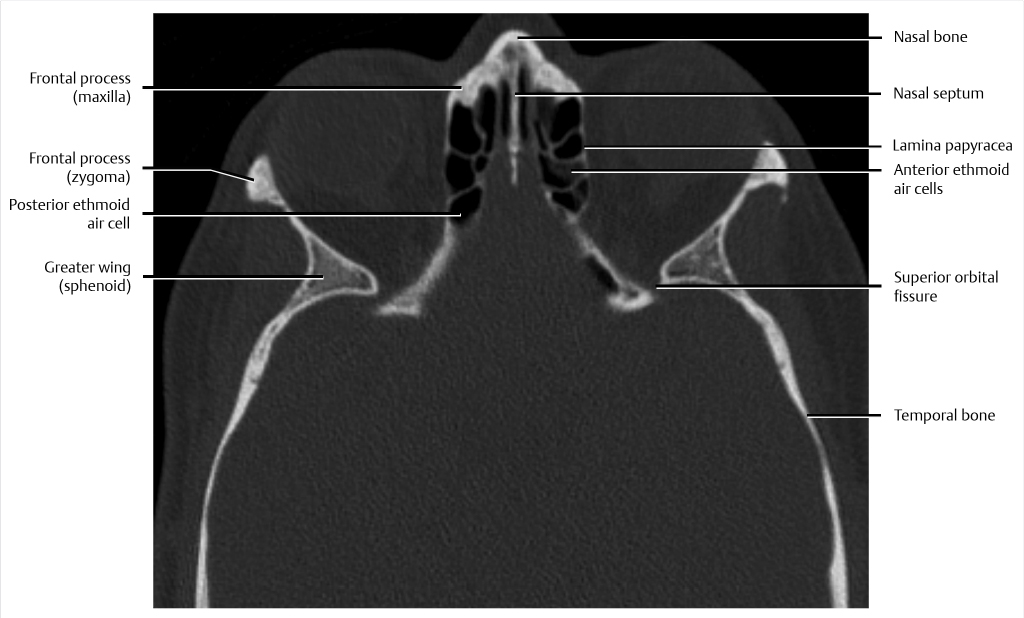
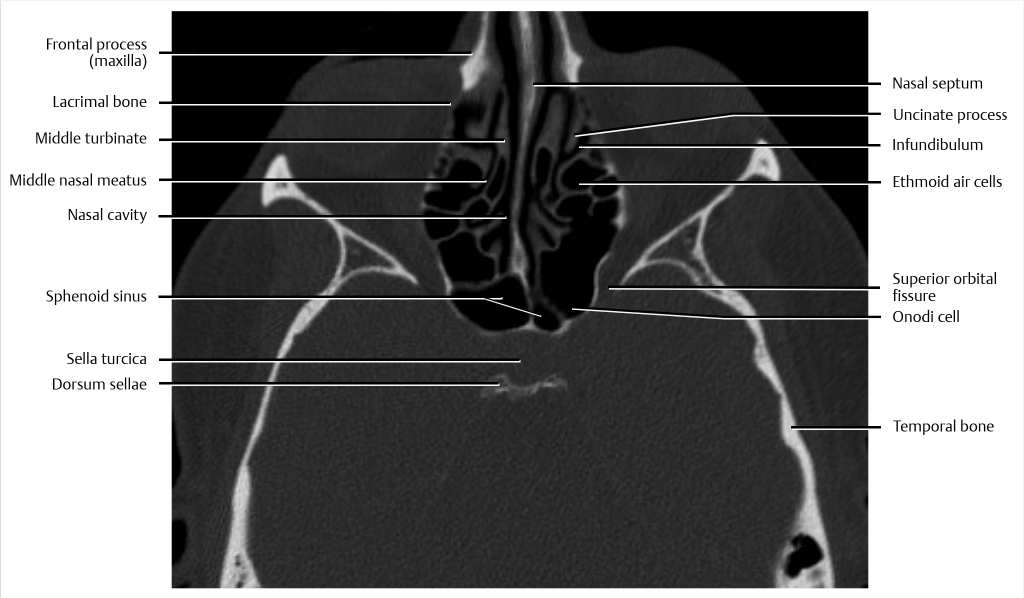
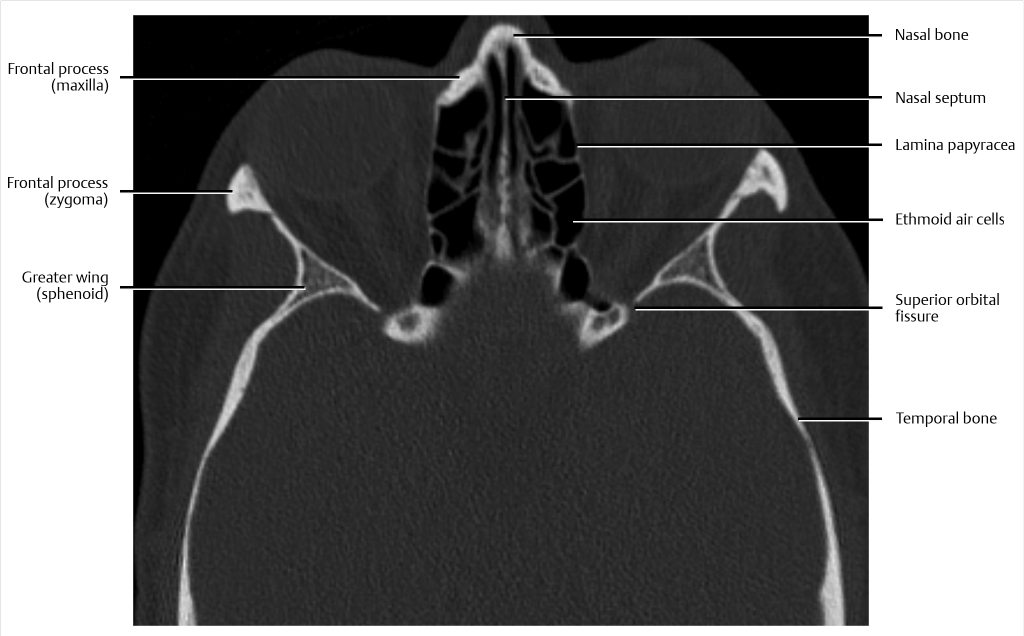
Fig. 8.7, ![]() Fig. 8.8). The skull base and paranasal sinuses are formed by the fusion of multiple bones, as shown. In the region of the anterior skull base, different compartments including the intracranial compartment, orbits, nasal cavity, and paranasal sinuses partly abut one another. These anatomic relationships are important and constitute different potential pathways of spread of pathology. CT is excellent for the evaluation of detailed skull base bone anatomy including major foramina and fissures. In this case, the superior orbital fissure is seen. This fissure or cleft is located between the lesser and greater wings of the sphenoid through which cranial nerves (III, IV, V1, VI) and the superior ophthalmic vein are transmitted to the orbit.
Fig. 8.8). The skull base and paranasal sinuses are formed by the fusion of multiple bones, as shown. In the region of the anterior skull base, different compartments including the intracranial compartment, orbits, nasal cavity, and paranasal sinuses partly abut one another. These anatomic relationships are important and constitute different potential pathways of spread of pathology. CT is excellent for the evaluation of detailed skull base bone anatomy including major foramina and fissures. In this case, the superior orbital fissure is seen. This fissure or cleft is located between the lesser and greater wings of the sphenoid through which cranial nerves (III, IV, V1, VI) and the superior ophthalmic vein are transmitted to the orbit.
![]() Fig. 8.9,
Fig. 8.9, ![]() Fig. 8.10,
Fig. 8.10, ![]() Fig. 8.11,
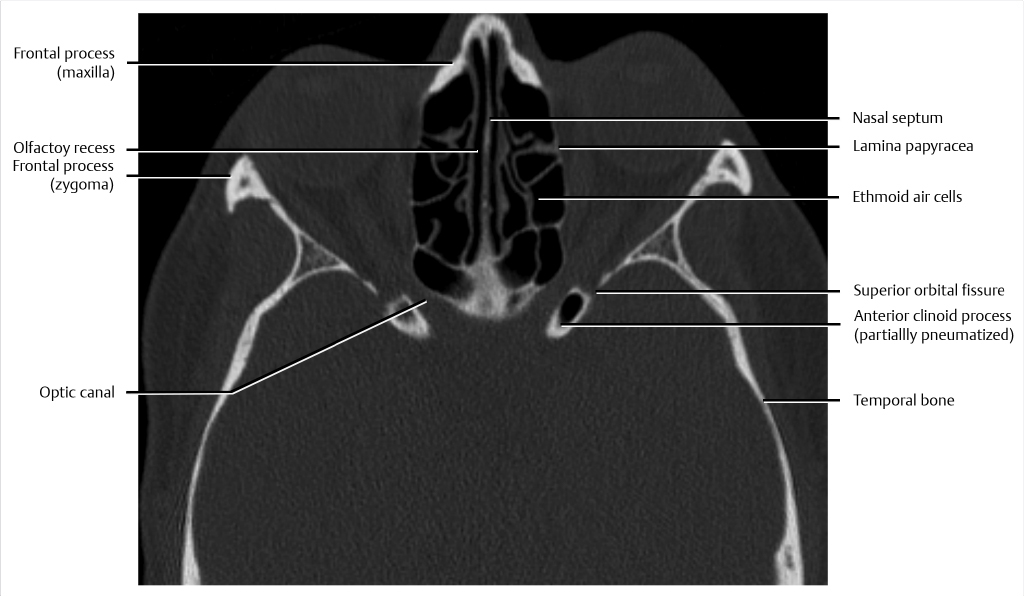
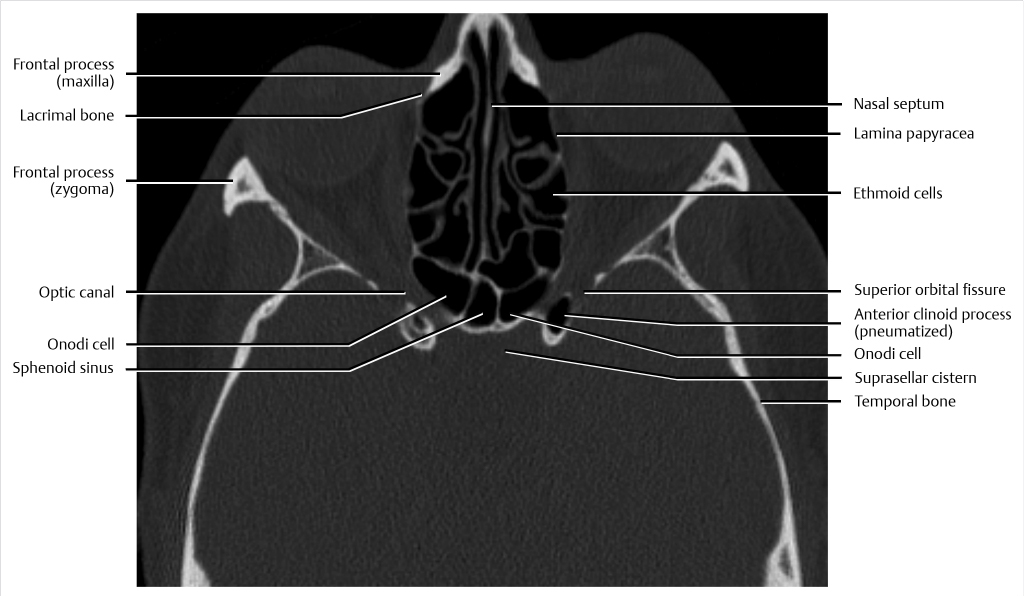
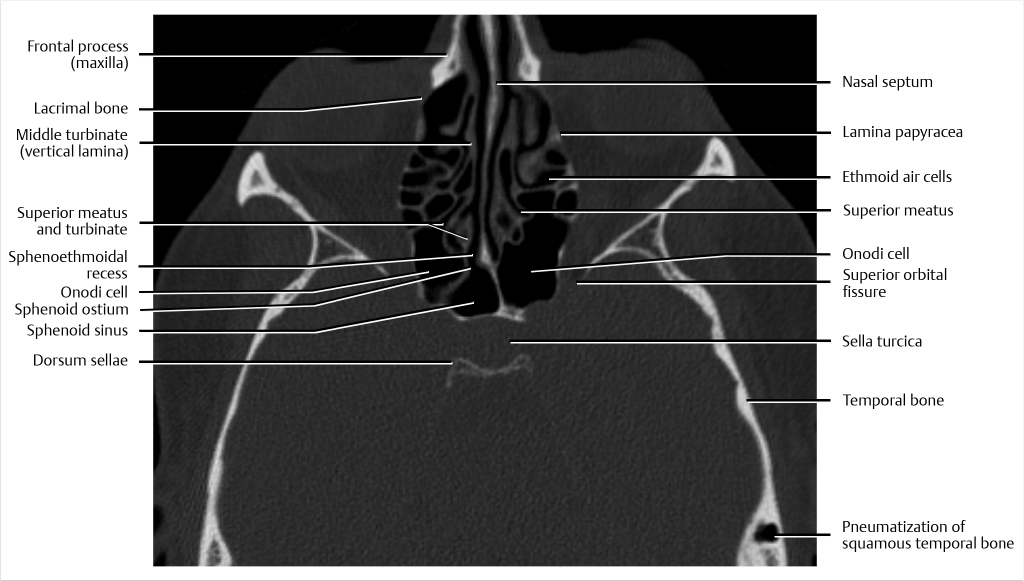
Fig. 8.11, ![]() Fig. 8.12). The skull base and paranasal sinuses are formed by the fusion of multiple bones, as shown. In the region of the anterior skull base, different compartments including the intracranial compartment, orbits, nasal cavity, and paranasal sinuses partly abut one another. These anatomic relationships are important and constitute different potential pathways of spread of pathology. CT is excellent for the evaluation of detailed skull base bone anatomy including major foramina and fissures. The superior orbital fissure is a cleft between the lesser and greater wings of the sphenoid through which cranial nerves (III, IV, V1, VI) and the superior ophthalmic vein traverse into the orbit. The optic nerve and ophthalmic artery pass through the optic canal. Variations such as pneumatization of the anterior clinoid process have an increased association with optic nerve exposure and dehiscence and are considered an indicator of optic nerve vulnerability during endoscopic sinus surgery.
Fig. 8.12). The skull base and paranasal sinuses are formed by the fusion of multiple bones, as shown. In the region of the anterior skull base, different compartments including the intracranial compartment, orbits, nasal cavity, and paranasal sinuses partly abut one another. These anatomic relationships are important and constitute different potential pathways of spread of pathology. CT is excellent for the evaluation of detailed skull base bone anatomy including major foramina and fissures. The superior orbital fissure is a cleft between the lesser and greater wings of the sphenoid through which cranial nerves (III, IV, V1, VI) and the superior ophthalmic vein traverse into the orbit. The optic nerve and ophthalmic artery pass through the optic canal. Variations such as pneumatization of the anterior clinoid process have an increased association with optic nerve exposure and dehiscence and are considered an indicator of optic nerve vulnerability during endoscopic sinus surgery.
![]() Fig. 8.13,
Fig. 8.13, ![]() Fig. 8.14,
Fig. 8.14, ![]() Fig. 8.15,
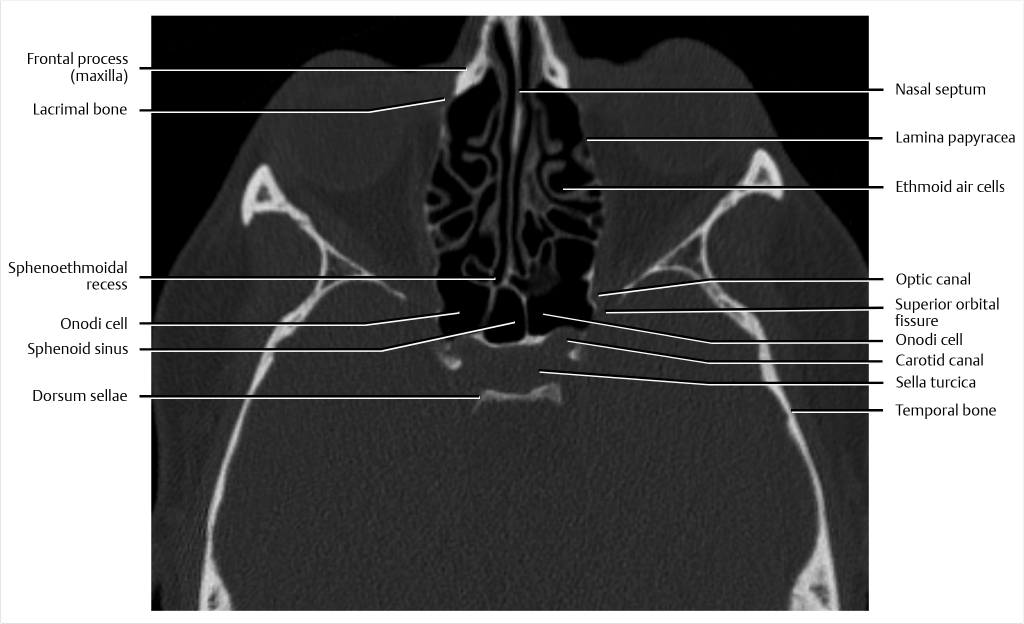
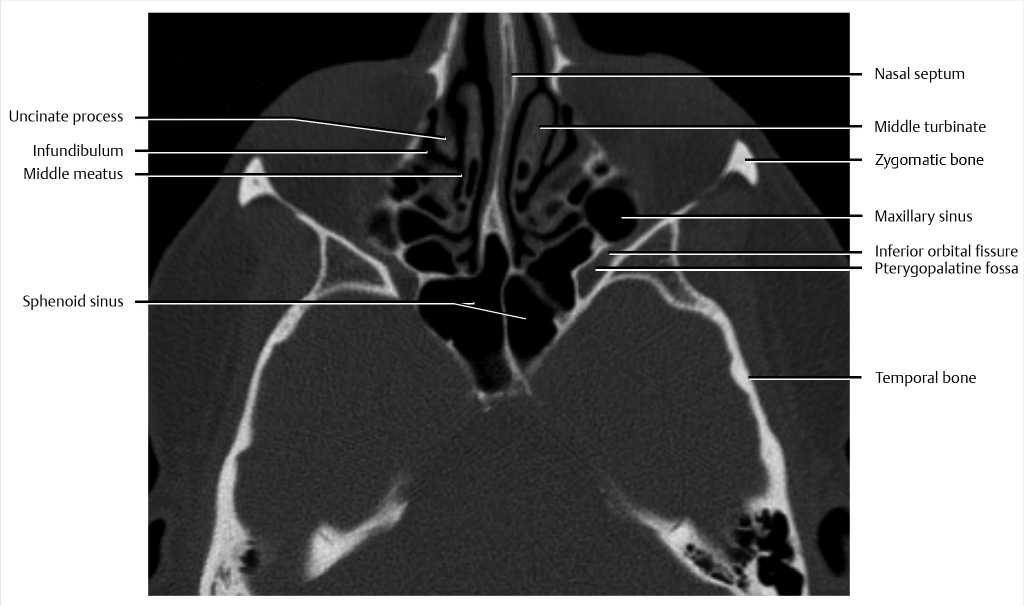
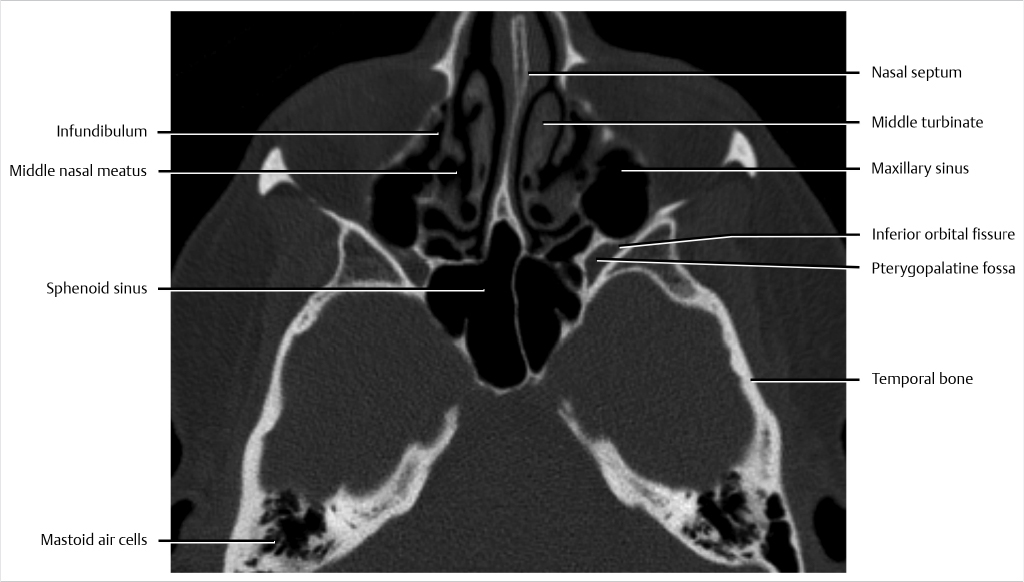
Fig. 8.15, ![]() Fig. 8.16). CT is excellent for the evaluation of detailed skull base bone anatomy including major foramina and fissures. The superior orbital fissure is a cleft between the lesser and greater wings of the sphenoid through which cranial nerves (III, IV, V1, VI) and the superior ophthalmic vein traverse into the orbit. The inferior orbital fissure transmits the zygomatic branch of V2 (maxillary division of trigeminal nerve) and the inferior ophthalmic vein. The inferior orbital fissure is also in continuity with the superior aspect of the pterygopalatine fossa (PPF), an important site of anatomic convergence of multiple neural pathways. Anatomic variations of the paranasal sinuses such as Onodi cells (well seen on coronal reformats) are important to recognize because there is potential for misidentification during endoscopic surgery that would put closely related critical structures, in particular the optic nerves, at risk for inadvertent surgical injury.
Fig. 8.16). CT is excellent for the evaluation of detailed skull base bone anatomy including major foramina and fissures. The superior orbital fissure is a cleft between the lesser and greater wings of the sphenoid through which cranial nerves (III, IV, V1, VI) and the superior ophthalmic vein traverse into the orbit. The inferior orbital fissure transmits the zygomatic branch of V2 (maxillary division of trigeminal nerve) and the inferior ophthalmic vein. The inferior orbital fissure is also in continuity with the superior aspect of the pterygopalatine fossa (PPF), an important site of anatomic convergence of multiple neural pathways. Anatomic variations of the paranasal sinuses such as Onodi cells (well seen on coronal reformats) are important to recognize because there is potential for misidentification during endoscopic surgery that would put closely related critical structures, in particular the optic nerves, at risk for inadvertent surgical injury.

![]() Fig. 8.17,
Fig. 8.17, ![]() Fig. 8.18,
Fig. 8.18, ![]() Fig. 8.19,
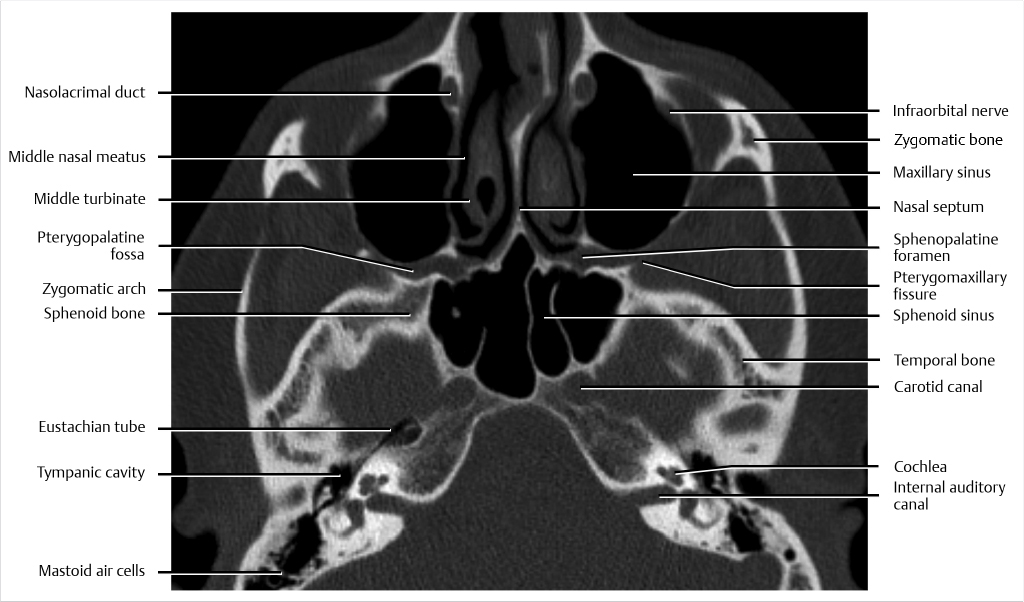
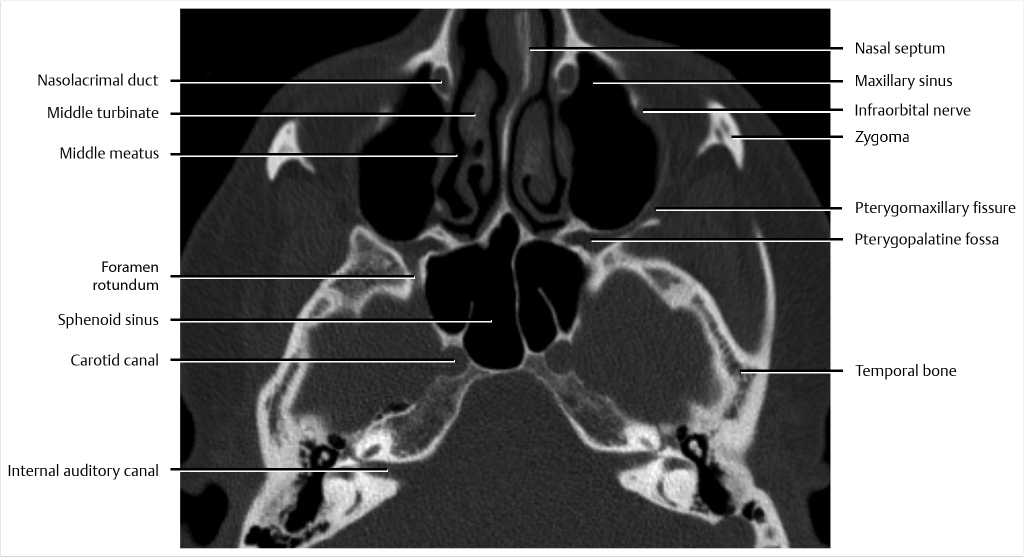
Fig. 8.19, ![]() Fig. 8.20). CT is excellent for the evaluation of detailed skull base bone anatomy including major foramina and fissures. The PPF is an important elongated, vertically oriented, predominantly fat-filled region located lateral to the posterior aspect of the nasal cavity that has an important relationship to the skull base and paranasal sinuses. The PPF is an important site of anatomic convergence of multiple neural pathways, and familiarity with this area is critical, particularly for evaluation of tumors where there is potential for perineural spread of tumor affecting treatment planning and management. At the lateral boundary of the PPF, there is an opening referred to as the pterygomaxillary fissure, an elongated vertical communication with the infratemporal fossa. The superior aspect of PPF is in continuity with the inferior orbital fissure and inferiorly, the PPF tapers into the greater palatine canal ultimately leading to the greater and lesser palatine foramina. Medially, the sphenopalatine foramen opens just posterior to the superior or middle meatus where the foramen is covered by mucosa. Posteriorly, the foramen rotundum communicates with the middle cranial fossa, transmitting the maxillary (V2) branch of the trigeminal nerve, artery of foramen rotundum, and emissary veins.
Fig. 8.20). CT is excellent for the evaluation of detailed skull base bone anatomy including major foramina and fissures. The PPF is an important elongated, vertically oriented, predominantly fat-filled region located lateral to the posterior aspect of the nasal cavity that has an important relationship to the skull base and paranasal sinuses. The PPF is an important site of anatomic convergence of multiple neural pathways, and familiarity with this area is critical, particularly for evaluation of tumors where there is potential for perineural spread of tumor affecting treatment planning and management. At the lateral boundary of the PPF, there is an opening referred to as the pterygomaxillary fissure, an elongated vertical communication with the infratemporal fossa. The superior aspect of PPF is in continuity with the inferior orbital fissure and inferiorly, the PPF tapers into the greater palatine canal ultimately leading to the greater and lesser palatine foramina. Medially, the sphenopalatine foramen opens just posterior to the superior or middle meatus where the foramen is covered by mucosa. Posteriorly, the foramen rotundum communicates with the middle cranial fossa, transmitting the maxillary (V2) branch of the trigeminal nerve, artery of foramen rotundum, and emissary veins.
![]() Fig. 8.21,
Fig. 8.21, ![]() Fig. 8.22,
Fig. 8.22, ![]() Fig. 8.23,
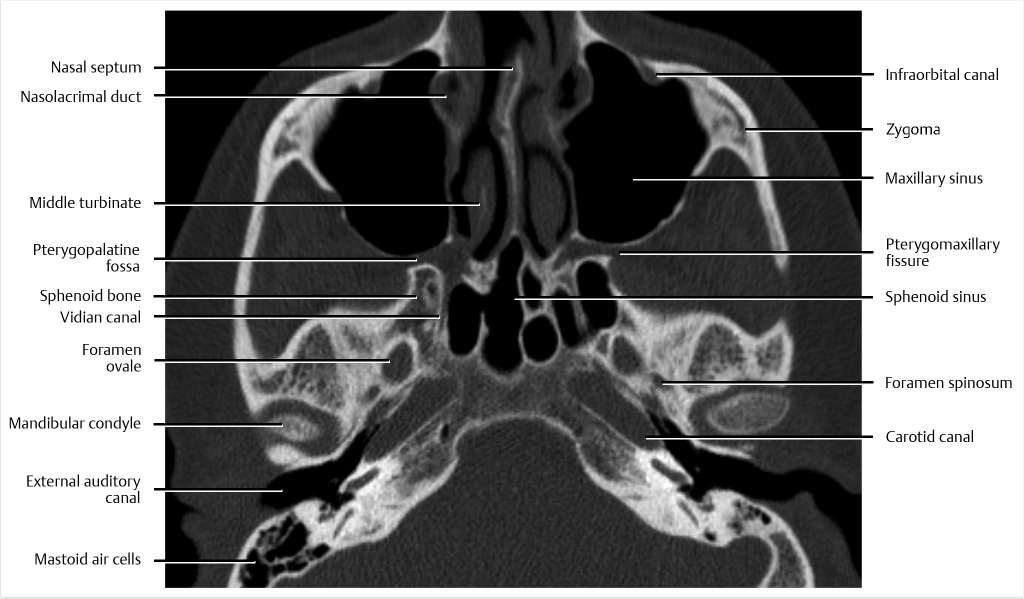
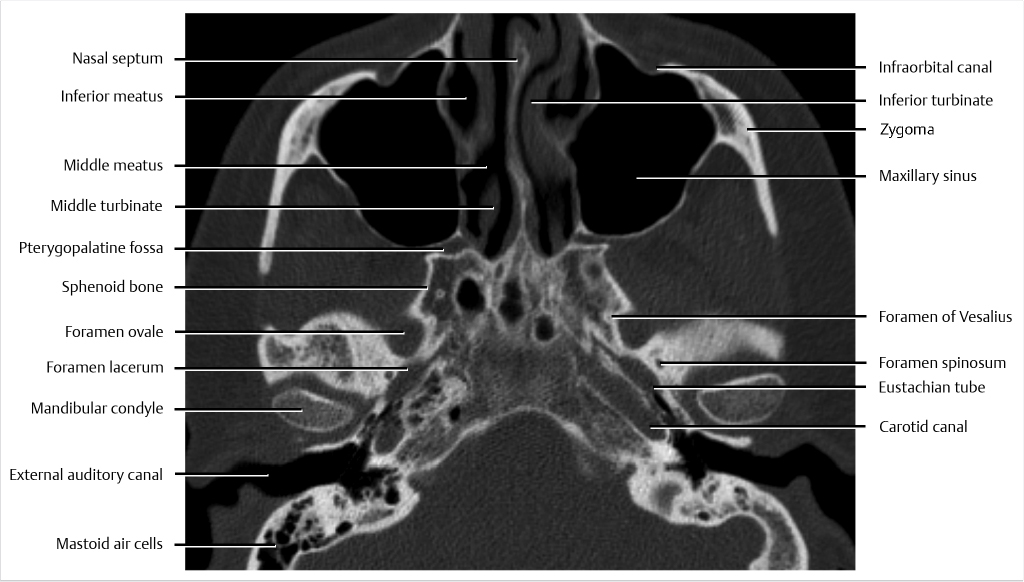
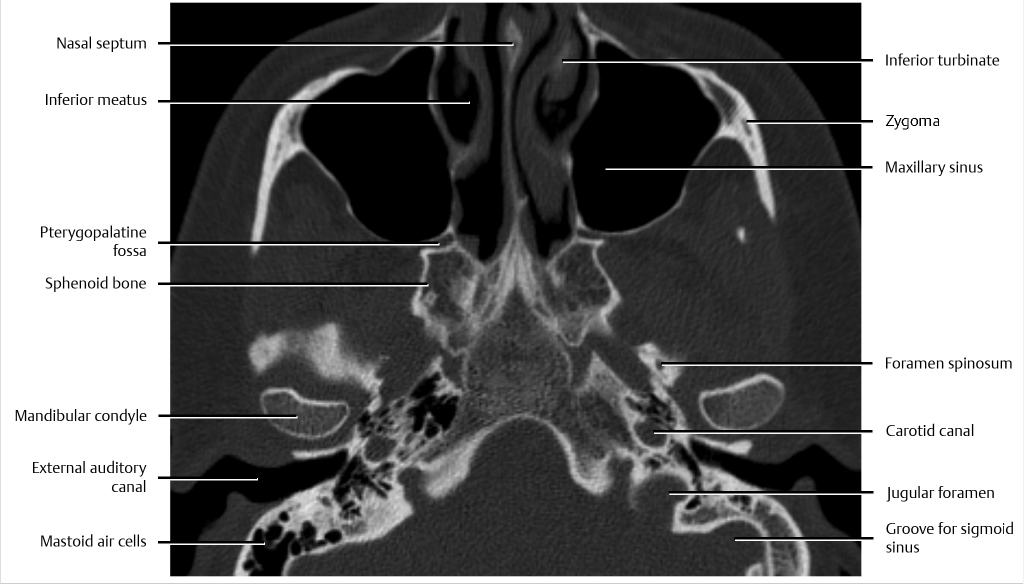
Fig. 8.23, ![]() Fig. 8.24). CT is excellent for the evaluation of detailed skull base bone anatomy including major foramina and fissures. The PPF is an important elongated, vertically oriented, predominantly fat-filled region located lateral to the posterior aspect of the nasal cavity that has an important relationship to the skull base and paranasal sinuses. The PPF is an important site of anatomic convergence of multiple neural pathways, and familiarity with this area is critical, particularly for evaluation of tumors where there is potential for perineural spread of tumor affecting treatment planning and management. At the lateral boundary of the PPF, there is an opening referred to as the pterygomaxillary fissure, an elongated vertical communication with the infratemporal fossa. The superior aspect of PPF is in continuity with the inferior orbital fissure and inferiorly, the PPF tapers into the greater palatine canal, ultimately leading to the greater and lesser palatine foramina. Medially, the sphenopalatine foramen opens just posterior to the superior or middle meatus where the foramen is covered by mucosa. Posteriorly, the foramen rotundum communicates with the middle cranial fossa, transmitting the maxillary (V2) branch of the trigeminal nerve, artery of foramen rotundum, and emissary veins. The Vidian (pterygoid) canal is also located posteriorly and extends to the foramen lacerum, transmitting the Vidian nerve. More posteriorly in the central skull base, another important foramen, foramen ovale, transmits the mandibular (V3) branch of the trigeminal nerve, lesser petrosal nerve, accessory meningeal branch of maxillary artery, and emissary vein, and provides a direct communication between the cranial cavity and the masticator space.
Fig. 8.24). CT is excellent for the evaluation of detailed skull base bone anatomy including major foramina and fissures. The PPF is an important elongated, vertically oriented, predominantly fat-filled region located lateral to the posterior aspect of the nasal cavity that has an important relationship to the skull base and paranasal sinuses. The PPF is an important site of anatomic convergence of multiple neural pathways, and familiarity with this area is critical, particularly for evaluation of tumors where there is potential for perineural spread of tumor affecting treatment planning and management. At the lateral boundary of the PPF, there is an opening referred to as the pterygomaxillary fissure, an elongated vertical communication with the infratemporal fossa. The superior aspect of PPF is in continuity with the inferior orbital fissure and inferiorly, the PPF tapers into the greater palatine canal, ultimately leading to the greater and lesser palatine foramina. Medially, the sphenopalatine foramen opens just posterior to the superior or middle meatus where the foramen is covered by mucosa. Posteriorly, the foramen rotundum communicates with the middle cranial fossa, transmitting the maxillary (V2) branch of the trigeminal nerve, artery of foramen rotundum, and emissary veins. The Vidian (pterygoid) canal is also located posteriorly and extends to the foramen lacerum, transmitting the Vidian nerve. More posteriorly in the central skull base, another important foramen, foramen ovale, transmits the mandibular (V3) branch of the trigeminal nerve, lesser petrosal nerve, accessory meningeal branch of maxillary artery, and emissary vein, and provides a direct communication between the cranial cavity and the masticator space.
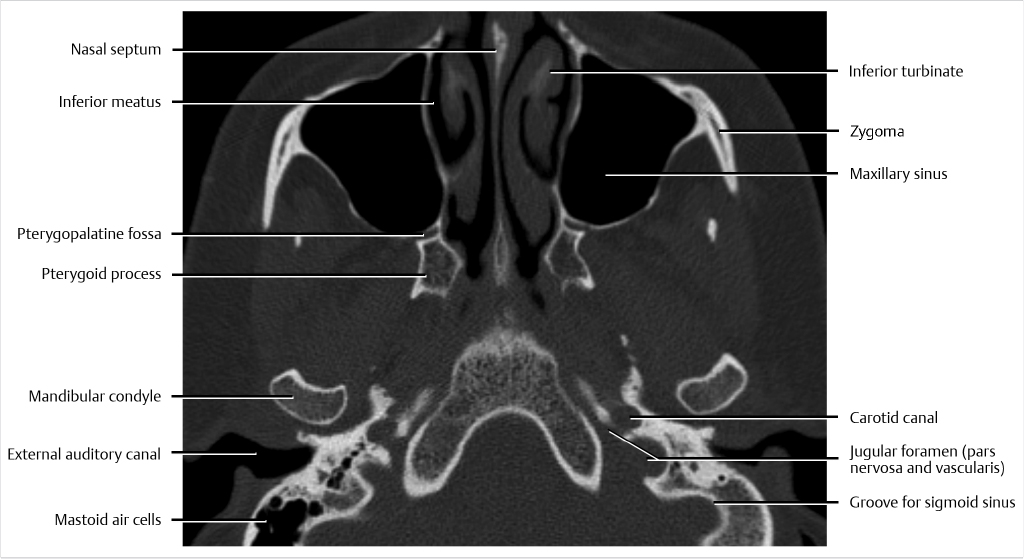
![]() Fig. 8.25,
Fig. 8.25, ![]() Fig. 8.26,
Fig. 8.26, ![]() Fig. 8.27,
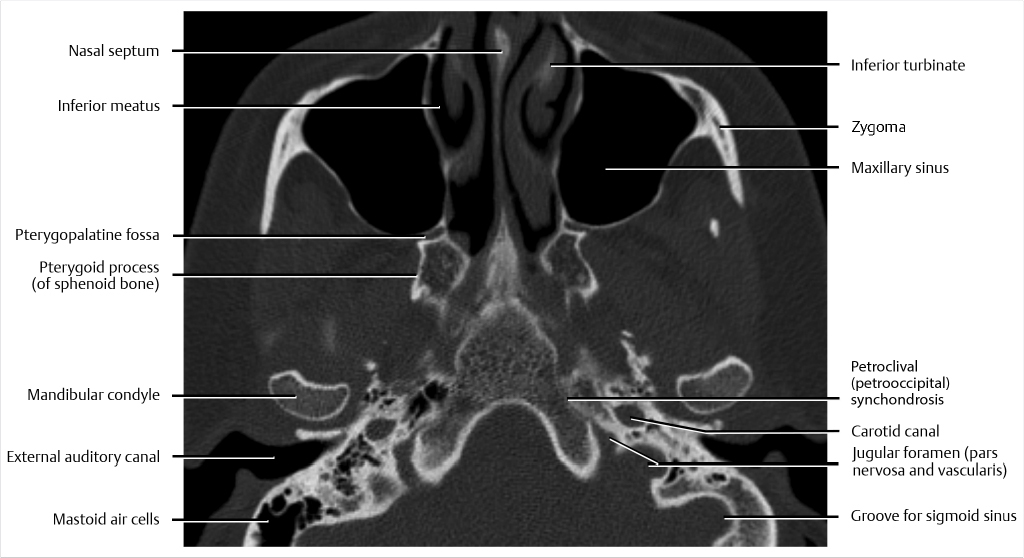
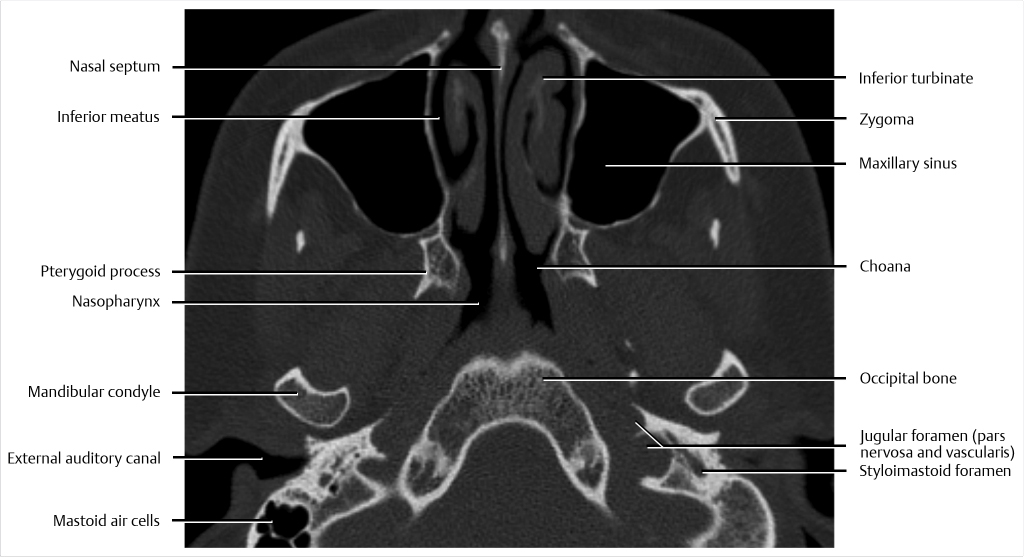
Fig. 8.27, ![]() Fig. 8.28). CT is excellent for the evaluation of detailed skull base bone anatomy including major foramina and fissures. Inferiorly, the PPF tapers into the greater palatine canal, ultimately leading to the greater and lesser palatine foramina. More posteriorly in the posterior skull base, the jugular foramen has two parts, the pars nervosa and pars vascularis, which are partly divided by the jugular spine. Medially and anteriorly, the pars nervosa contains cranial nerve IX, Jacobson nerve, and inferior petrosal sinus. Laterally and more posteriorly, the larger pars vascularis contains cranial nerves X and XI, Arnold nerve, jugular bulb, and posterior meningeal artery. The stylomastoid foramen, located between the mastoid tip and styloid process, is the site of passage of cranial nerve VII from the temporal bone to the extracranial compartment.
Fig. 8.28). CT is excellent for the evaluation of detailed skull base bone anatomy including major foramina and fissures. Inferiorly, the PPF tapers into the greater palatine canal, ultimately leading to the greater and lesser palatine foramina. More posteriorly in the posterior skull base, the jugular foramen has two parts, the pars nervosa and pars vascularis, which are partly divided by the jugular spine. Medially and anteriorly, the pars nervosa contains cranial nerve IX, Jacobson nerve, and inferior petrosal sinus. Laterally and more posteriorly, the larger pars vascularis contains cranial nerves X and XI, Arnold nerve, jugular bulb, and posterior meningeal artery. The stylomastoid foramen, located between the mastoid tip and styloid process, is the site of passage of cranial nerve VII from the temporal bone to the extracranial compartment.


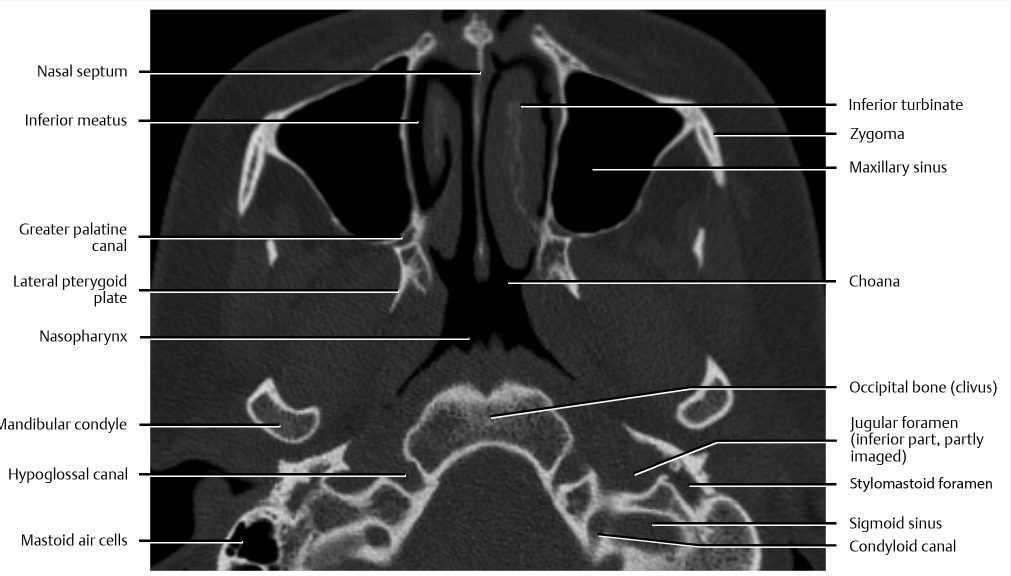
![]() Fig. 8.29,
Fig. 8.29, ![]() Fig. 8.30,
Fig. 8.30, ![]() Fig. 8.31,
Fig. 8.31, ![]() Fig. 8.32). CT is excellent for the evaluation of detailed skull base bone anatomy including major foramina and fissures. Inferiorly, the PPF tapers into the greater palatine canal, ultimately leading to the greater and lesser palatine foramina. The greater palatine foramen transmits the greater palatine nerve and descending palatine vessels. The lesser palatine foramen transmits the lesser palatine nerves. Although commonly single, there can be two or rarely more than two lesser palatine foramina. More posteriorly in the posterior skull base, the hypoglossal canal transmits cranial nerve XII. The stylomastoid foramen, located between the mastoid tip and styloid process, is the site of passage of cranial nerve VII from the temporal bone to the extracranial compartment. The condyloid (or posterior condylar) canals transmit emissary veins and provide an anastomosis between the jugular bulb and the suboccipital venous plexus. These are among the largest emissary foramina in the skull and should not be misinterpreted as pathology.
Fig. 8.32). CT is excellent for the evaluation of detailed skull base bone anatomy including major foramina and fissures. Inferiorly, the PPF tapers into the greater palatine canal, ultimately leading to the greater and lesser palatine foramina. The greater palatine foramen transmits the greater palatine nerve and descending palatine vessels. The lesser palatine foramen transmits the lesser palatine nerves. Although commonly single, there can be two or rarely more than two lesser palatine foramina. More posteriorly in the posterior skull base, the hypoglossal canal transmits cranial nerve XII. The stylomastoid foramen, located between the mastoid tip and styloid process, is the site of passage of cranial nerve VII from the temporal bone to the extracranial compartment. The condyloid (or posterior condylar) canals transmit emissary veins and provide an anastomosis between the jugular bulb and the suboccipital venous plexus. These are among the largest emissary foramina in the skull and should not be misinterpreted as pathology.
![]() Fig. 8.33,
Fig. 8.33, ![]() Fig. 8.34,
Fig. 8.34, ![]() Fig. 8.35,
Fig. 8.35, ![]() Fig. 8.36). CT is excellent for the evaluation of detailed skull base bone anatomy including major foramina and fissures as well as other structures at the skull base. The greater palatine foramen transmits the greater palatine nerve and descending palatine vessels. The lesser palatine foramen transmits the lesser palatine nerves. Although commonly single, there can be two or rarely more than two lesser palatine foramina. There are important relationships of the skull base to adjacent spaces and cavities, including the nasopharynx. Seen here in the nasopharynx is the torus tubarius, the cartilaginous end of the Eustachian tube, and the fossa of Rosenmüller (or pharyngeal recess).
Fig. 8.36). CT is excellent for the evaluation of detailed skull base bone anatomy including major foramina and fissures as well as other structures at the skull base. The greater palatine foramen transmits the greater palatine nerve and descending palatine vessels. The lesser palatine foramen transmits the lesser palatine nerves. Although commonly single, there can be two or rarely more than two lesser palatine foramina. There are important relationships of the skull base to adjacent spaces and cavities, including the nasopharynx. Seen here in the nasopharynx is the torus tubarius, the cartilaginous end of the Eustachian tube, and the fossa of Rosenmüller (or pharyngeal recess).
![]() Fig. 8.37,
Fig. 8.37, ![]() Fig. 8.38,
Fig. 8.38, ![]() Fig. 8.39,
Fig. 8.39, ![]() Fig. 8.40). CT is excellent for the evaluation of detailed skull base bone anatomy including major foramina and fissures as well as other structures at the skull base.
Fig. 8.40). CT is excellent for the evaluation of detailed skull base bone anatomy including major foramina and fissures as well as other structures at the skull base.
8.2.2 Coronal Image Set
Coronal Computed Tomography (No Contrast)
![]() Fig. 8.41,
Fig. 8.41, ![]() Fig. 8.42,
Fig. 8.42, ![]() Fig. 8.43,
Fig. 8.43, ![]() Fig. 8.44). The skull base and paranasal sinuses are formed by the fusion of multiple bones, as shown. The anterior skull base can be broadly described as constituting the floor of the anterior cranial fossa and the roof of the nose, ethmoid air cells, and orbits. These anatomic relationships are important and constitute different potential pathways of spread of pathology.
Fig. 8.44). The skull base and paranasal sinuses are formed by the fusion of multiple bones, as shown. The anterior skull base can be broadly described as constituting the floor of the anterior cranial fossa and the roof of the nose, ethmoid air cells, and orbits. These anatomic relationships are important and constitute different potential pathways of spread of pathology.
![]() Fig. 8.45,
Fig. 8.45, ![]() Fig. 8.46,
Fig. 8.46, ![]() Fig. 8.47,
Fig. 8.47, ![]() Fig. 8.48). CT is excellent for the evaluation of detailed skull base and paranasal sinus bony anatomy. The horizontal central part of the roof of the nasal cavity is formed by the cribriform plate. The cribriform plate has a medial lamella inferiorly and medially and a lateral lamella that is vertical or slanted. The lateral lamella of the cribriform plate is the thinnest structure in the skull base and as such represents a site of potential breach or injury during surgery. The fovea ethmoidalis forms the roof of the ethmoid labyrinth. The symmetry, slanting, and depth of the cribriform plate and fovea ethmoidalis are also important for surgical planning and well demonstrated on coronal CT images. Different anatomic variants of the paranasal sinuses, including Agger nasi cells and frontal cells, are well seen on coronal and sagittal reformats. The infraorbital canal transmits the infraorbital nerve, a branch of V2 (maxillary division of trigeminal nerve).
Fig. 8.48). CT is excellent for the evaluation of detailed skull base and paranasal sinus bony anatomy. The horizontal central part of the roof of the nasal cavity is formed by the cribriform plate. The cribriform plate has a medial lamella inferiorly and medially and a lateral lamella that is vertical or slanted. The lateral lamella of the cribriform plate is the thinnest structure in the skull base and as such represents a site of potential breach or injury during surgery. The fovea ethmoidalis forms the roof of the ethmoid labyrinth. The symmetry, slanting, and depth of the cribriform plate and fovea ethmoidalis are also important for surgical planning and well demonstrated on coronal CT images. Different anatomic variants of the paranasal sinuses, including Agger nasi cells and frontal cells, are well seen on coronal and sagittal reformats. The infraorbital canal transmits the infraorbital nerve, a branch of V2 (maxillary division of trigeminal nerve).
Related posts:
![]() Neuroendovascular Procedures for Skull Base Neoplasia
Neuroendovascular Procedures for Skull Base Neoplasia
 Open and Endoscopic Approaches to the Sinonasal Cavity and Skull Base
Open and Endoscopic Approaches to the Sinonasal Cavity and Skull Base
![]() Posttreatment Appearance Following Skull Base Therapy
Posttreatment Appearance Following Skull Base Therapy
 Cerebellopontine Angle and Jugular Fossa
Cerebellopontine Angle and Jugular Fossa
 Sellar, Parasellar, and Clival Region
Sellar, Parasellar, and Clival Region
 Anterior Cranial Fossa, Nasal Cavity, and Paranasal Sinuses
Anterior Cranial Fossa, Nasal Cavity, and Paranasal Sinuses
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine