CHAPTER 17 Cross-sectional investigations, nuclear medicine and ultrasound of the small and large bowel

















Introduction
Most abdominal imaging is performed to investigate general abdominal symptoms, such as pain, weight loss, bloating or abdominal distension. Abdominal imaging involves a multitude of complex investigations to the uninitiated. Ultrasound, computed tomography (CT), magnetic resonance imaging (MRI) and radionuclide scanning are all important adjuncts to first line imaging: the abdominal radiograph. They are complementary to each other and the majority of clinical questions can be answered by cross- sectional imaging. Occasionally specialist investigations will be required e.g. indium-111 labelled white cell nuclear scintigraphy when the other imaging modalities have been negative and there are ongoing clinical symptoms or concern. Each investigative method is appropriate for certain clinical questions, when used appropriately it will help make an accurate diagnosis, preventing any treatment delays. To understand the role of each imaging modality you must understand the principle technique, including its value and limitations.
Evidence-based medicine can be defined as the integration of best available research with clinical expertise and patient values (Erturk et al., 2006). You can apply evidence-based practice to any clinical discipline using five basic principles:
Ultrasound
The basic essential component of an ultrasound probe is the piezoelectric (PZE) crystal in a shape of a rectangle or disk. When an alternating (AC) current is applied to the crystal, it expands and contracts with the same frequency: this is the ‘piezoelectric effect’. This produces sound waves or echoes. The echoes are transmitted undergoing ‘reflection’, returning at different velocities depending on the media the echoes have encountered within the body. Different tissues will have different acoustic impedance. The proportion of energy (or sound) reflected and transmitted depends on the acoustic impedances of the two materials. In physics terms, the acoustic impedance of a material is defined as the product of the density of the material and the velocity of the sound within it. The greater the acoustic impedance mismatches between two materials the greater the fraction of sound which is reflected and thus imaging is limited. The reflected/returning sound waves act on the PZE crystal in the ultrasound probe to produce an electric signal. The probe is connected to a powerful computer processor that converts the electrical signal into a cross-sectional image. The images are captured in real time and it can show the solid organs and the movement and flow through blood vessels using a special technique of Doppler ultrasound. The image is then displayed on a monitor and may be stored or printed.
The properties of ultrasound are unique. Unlike x-rays or light waves, which can travel through a vacuum, sound waves require a material medium to travel through and thus cannot penetrate air gaps. Ultrasound cannot image through bone or large collections of air. There is also a high acoustic impedance mismatch between the patient’s skin and the probe. This is overcome by the use of ultrasound scanning gel. The advantages and limitations of ultrasound as an imaging modality are outlined in Boxes 17.1 and 17.2.












Doppler ultrasound
The combination of two-dimensional ultrasound imaging with Doppler ultrasound is known as duplex ultrasound. Duplex is an important technique for the examination of arteries and veins.
Applied terminology
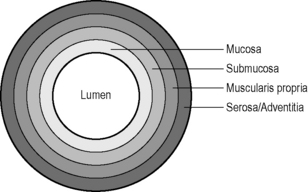
Hypoechoic: dark gray, nearly black, e.g. fat, muscularis propria of the bowel wall.
Isoechoic: gray lesion, e.g. liver substance or gut wall.

Patient preparation
Ultrasound of the kidneys
To evaluate the bladder, it must be distended fully. This is achieved by drinking one litre of water or more, an hour before the examination. If the patient is catheterized it should be clamped off, again to fill the bladder. If the bladder is only partially filled, then only comment can be made on any gross/large abnormalities. Small lesions cannot be confidently detected.
Ultrasound of the Bowel
Ultrasound of small and large bowel
Acute appendicitis in experienced hands is usually diagnosed on history, physical examination and laboratory investigations. The aim of imaging is either to confirm or refute the diagnosis; however, if the appendix is not visualized then appendicitis cannot be excluded. In a female, diagnoses which mimic appendicitis include enlarged ovarian cysts or torsion of the ovaries. Thickening of the wall of a normal appendix wall to 6 mm (3 mm or less is normal) is suggestive of appendicitis (Guillerman and Ng, 2005). Other features include non-compressibility and round in cross-section rather than oval.
Ultrasound of the bowel can be used for bowel obstruction and in Crohn’s disease. Bowel obstruction





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


