, Joungho Han2, Man Pyo Chung3 and Yeon Joo Jeong4
(1)
Department of Radiology Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea, Republic of (South Korea)
(2)
Department of Pathology Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea, Republic of (South Korea)
(3)
Department of Medicine Division of Pulmonary and Critical Care Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea, Republic of (South Korea)
(4)
Department of Radiology, Pusan National University Hospital, Busan, Korea, Republic of (South Korea)
Abstract
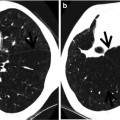
CT halo sign is a CT finding of ground-glass opacity surrounding a nodule or mass. It was first described as a sign of hemorrhage around foci of invasive pulmonary aspergillosis [1] (Fig. 6.1).
Definition
CT halo sign is a CT finding of ground-glass opacity surrounding a nodule or mass. It was first described as a sign of hemorrhage around foci of invasive pulmonary aspergillosis [1] (Fig. 6.1).
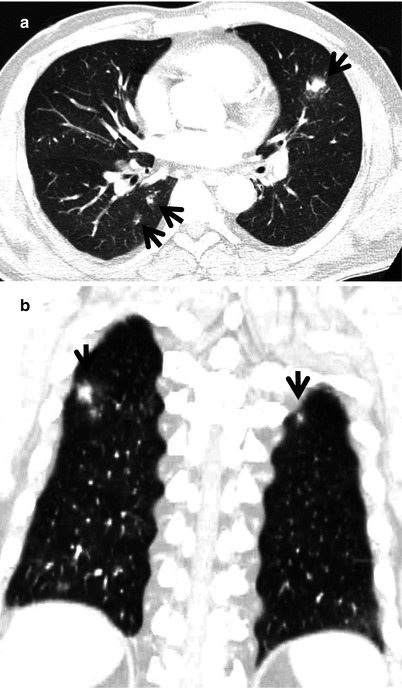
Fig. 6.1
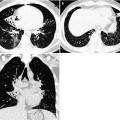
Toxocara canis and its larva migration in a 66-year-old man with colon cancer who had a history of raw cow liver intake. (a) Lung window of CT scan (2.5-mm section thickness) obtained at lower lobar bronchia level shows nodules (arrows) with surrounding halo sign in both lungs. (b) Coronal reformatted (2.0-mm section thickness) CT scan also demonstrates nodules (arrows) with halo sign
Diseases Causing the Sign
The halo sign is nonspecific and may be caused by several pathologic processes: hemorrhagic pulmonary nodules [2], tumor cell infiltration, and non-hemorrhagic inflammatory lesions. Hemorrhagic pulmonary nodules may occur in infectious diseases including angioinvasive pulmonary aspergillosis (Fig. 6.2), mucormycosis, and candidiasis and noninfectious diseases including antineutrophil cytoplasmic antibody (ANCA)-associated granulomatous vasculitis and primary and metastatic hemorrhagic tumors (Figs. 6.3 and 6.4). The hemorrhagic nodule can also be found in a patient with pulmonary endometriosis with catamenial hemorrhage [3, 4] (Fig. 6.5). Tumor cell infiltrations in lung adenocarcinomas, bronchus-associated lymphoid tissue (BALT) lymphoma, and pulmonary metastatic neoplasm may appear with the halo sign. Eosinophilic lung disease [5] (Fig. 6.1) and organizing pneumonia are representative of inflammatory lesions showing the halo sign (Table 6.1) [4].
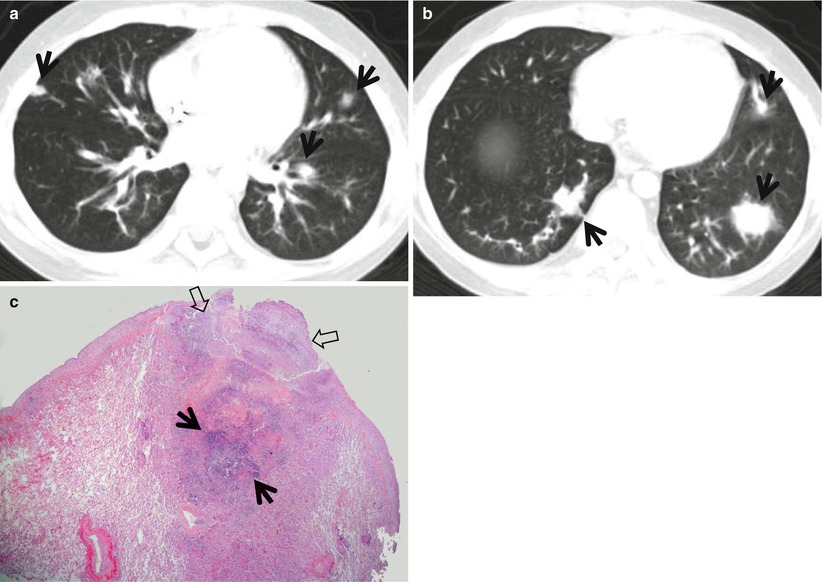

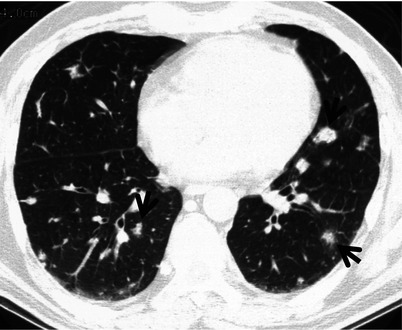
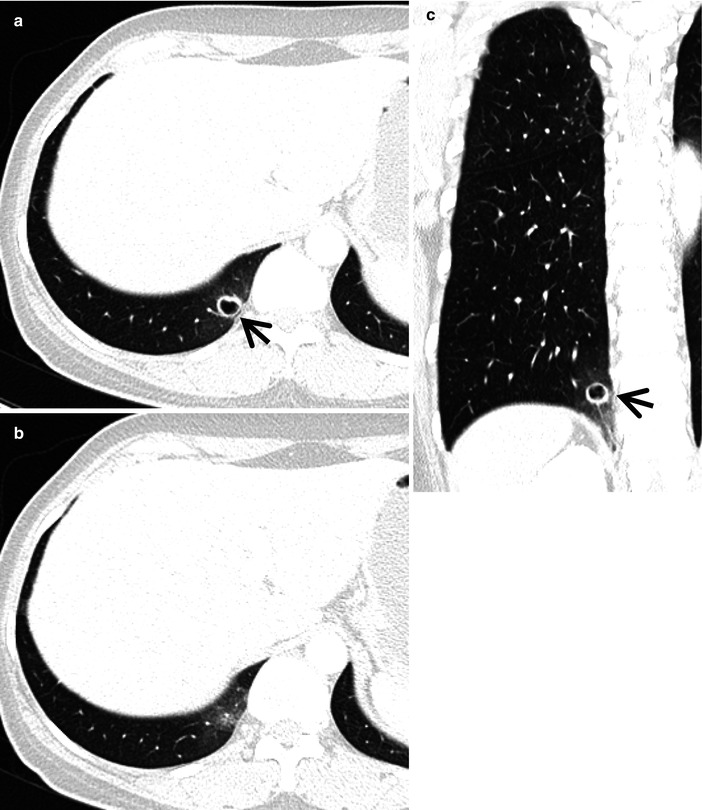
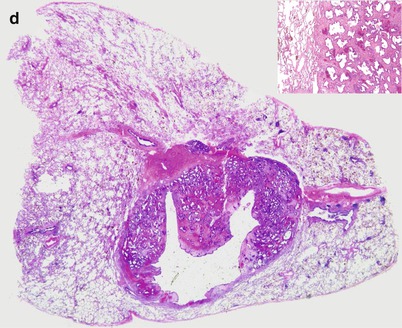
Fig. 6.2
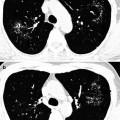
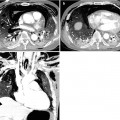
Invasive pulmonary aspergillosis in an 11-year-old boy with acute lymphocytic leukemia and neutropenia. (a, b) Lung window of CT (5.0-mm section thickness) scans obtained at levels of the inferior pulmonary vein (a) and liver dome (b), respectively, shows nodules (arrows) with halo sign in both lungs. Also note ground-glass opacity along bronchovascular bundles. (c) High-magnification photomicrograph of pathologic specimen obtained from the left lower lobe with wedge resection by using video-assisted thoracoscopic surgery discloses necrotic abscess containing blue area of fungal colonization (arrows) in central portion of lesion. Fungal organisms extend to pleural space (open arrows)
Fig. 6.3
Hemorrhagic metastasis in a 52-year-old woman with renal cell carcinoma. Lung window of CT (5.0-mm section thickness) scan obtained at level of the interior pulmonary vein shows multiple solid nodules surrounded by ground-glass opacity, suggesting hemorrhagic metastasis
Fig. 6.4
Nodules with halo sign in a 28-year-old man with melanoma. Lung window of CT (5.0-mm section thickness) scan obtained at level of the interior pulmonary vein shows multiple variable-sized nodules (arrows) having surrounding halo (hemorrhagic metastases)
Fig. 6.5
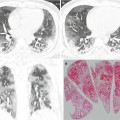
Pulmonary endometriosis showing halo sign in a 46-year-old woman. (a, b) Lung window of consecutive CT scans (2.5-mm section thickness) obtained at levels of liver dome shows a cystic lesion (arrow) of eccentric wall thickness depicting surrounding ground-glass opacity halo in the right lung base. (c) Coronal reformatted (2.0-mm section thickness) image demonstrates cystic lesion with halo sign (arrow). (d) High-magnification (×100) photomicrograph of pathologic specimen obtained from the right lower lobe with wedge resection by using video-assisted thoracoscopic surgery discloses a nodule composed of many well-formed endometrial glands and admixed stroma. Also note a large dilated gland-forming cyst within central portion of nodule. Inset: stroma is pale pink and is composed of bland-looking oval or spindle cells (×200)
Table 6.1
Common diseases manifesting as CT halo sign
Disease | Key points for differential diagnosis |
|---|---|
Infectious disease | |
Angioinvasive pulmonary aspergillosis | Nodules with a GGO, wedge-shaped pleural-based areas of consolidation |
Mucormycosis | Nodules and masses with CT and reversed halo |
Candidiasis | |
ANCA-associated granulomatous vasculitis | Multiple, bilateral, subpleural nodules or masses |
Hemorrhagic metastasis | Multiple nodules with GGO halo, varying in size |
Pulmonary endometriosis | Focal consolidation and GGO during menstruation |
Eosinophilic lung disease | Migrating multifocal subpleural nodules with GGO halo |
Distribution
The nodule and halo sign usually show random distribution without specific zonal, central–peripheral, or bronchovascular distribution. The nodule and halo sign may show subpleural distribution in angioinvasive pulmonary aspergillosis, metastatic hemorrhagic tumors, and non-hemorrhagic pulmonary metastatic neoplasms.
Clinical Considerations
Angioinvasive pulmonary aspergillosis is seen in neutropenic subjects with immunosuppression (absolute neutrophil count, <500/L). ANCA-associated granulomatous vasculitis is usually associated with clinical presentation that included acute glomerulonephritis, chronic refractory sinusitis, or rhinorrhea. Serologic test including cytoplasmic ANCA is performed for the diagnosis of the disease. Catamenial hemorrhage occurs at the time of patient menstruation. Eosinophilic lung disease is usually seen in patients who have intake history of freshwater crabs [6] or raw cow liver [7].
Key Points for Differential Diagnosis
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


