105 The differential diagnosis of cystic peritoneal masses is broad. Mesenteric, omental, and retroperitoneal cysts derive from the same embryologic structures. The term mesenteric cyst is often used to refer to cysts that do not connect to the retroperitoneum. Two frequent types of mesenteric cysts are of lymphatic and mesothelial origin. These differ in mode of presentation. Lymphangiomas predominate in boys. They can present with acute abdominal pain and often are attached to adjacent structures such as bowel. Unlike simple lymphatic cysts, they can be aggressive and recur if incompletely resected. They are more common in the mesentery in childhood and occur in the retroperitoneum during adulthood. Internal septations are usually present. The wall and the septations usually enhance. Lymphangiomas could be of similar density, less dense or more dense than fluid on computed tomography (CT). On magnetic resonance imaging (MRI), they are occasionally hyperintense on T1-weighted magnetic resonance images (T1WI) secondary to hemorrhage or fat.1–3 Cysts of mesothelial origin are seen more commonly in young and middle-aged women, presenting with indolent symptoms. Mesothelial cysts differ from lymphangiomas in that they have no internal septations and are never hyperintense on T1WI.3 Benign cystic mesothelioma (also known as peritoneal inclusion cyst) often arises from the pelvis, and is associated with a history of pelvic surgery, endometriosis, or pelvic inflammatory disease. It is not associated with asbestos exposure. Benign cystic mesothelioma is typically multiloculated in appearance. Unlike simple mesothelial cysts, they can be aggressive and recur if incompletely resected.2,4
Cystic Peritoneal and Retroperitoneal Masses
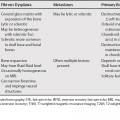
Cystic Peritoneal Masses
Lymphangiomas
Mesothelial Cysts
Enteric Cysts
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


