7 Cysts and Intracystic Tumors Breast cysts are usually the result of degenerative fibrocystic changes in the glandular breast tissue (Table 7.1). They are the most common palpable breast masses for which women seek medical attention (Table 7.2). In addition to fibrosis and intraductal proliferation, the pathogenesis involves an increase in secretory activity leading to fluid retention, ductal dilatation, and cyst formation. Cysts more than 2 mm in diameter are called macrocysts (Fig. 7.1), and those smaller than 2 mm are called micro-cysts (Fig. 7.2). Aspiration is warranted only in patients with clinical symptoms or suspected intracystic proliferation (Table 7.3). The correct interpretation of a sonogram often depends on the ultrasonographic technique, but when technique is optimal, most breast cysts can be confidently diagnosed (Table 7.4). The four criteria for diagnosis are round or oval shape, anechogenicity, circumscribed margins, and posterior acoustic enhancement (Fig. 7.1). Cysts do not augment sound transmission, although they may appear to do so; they merely attenuate the sound less than the solid surrounding tissues. Because the ultrasound system’s time gain compensation (TGC) corrects for the attenuation of the tissues adjacent to the cyst, there is an apparent enhancement or brightening of echoes deep to the cyst. The tangential incidence of the ultrasound beam on the smooth side walls of the cyst, along with the impedance mismatch between the cyst fluid and adjacent tissues, causes refractive effects that produce an edge shadow emanating from each side of the cyst. With a low-frequency transducer (< 7 MHz) and poor lateral resolution, it can be difficult to confirm the sharp thin lateral walls of a simple cyst. Cysts may be solitary or multiple and may occur in one or both breasts (Figs. 7.1–7.3 a–c). They may be unilocular or have thin internal septations (Fig. 7.4 a, b). Numerous small cysts or microcysts may be closely aggregated in a bunch-of-grapes pattern (Fig. 7.2). Cysts often contain small calcifications, punctate echoes that fall to the dependent portion of cysts (Fig. 7.5 a, b). The surrounding breast parenchyma may show increased echogenicity and sound attenuation, correlating with fibrotic and chronic inflammatory changes. The increased density of the tissues surrounding a cyst may obscure it on mammograms.
Clinical Significance
Diagnostic Criteria
Simple Cysts
|
|
|
 Imbalance between secretion and reabsorption in the lactiferous ducts
Imbalance between secretion and reabsorption in the lactiferous ducts Duct obstruction with retained secretions due to stromal fibrosis or ductal proliferation, usually involving the terminal ducts and ductules
Duct obstruction with retained secretions due to stromal fibrosis or ductal proliferation, usually involving the terminal ducts and ductules Hormonal dysfunction as in fibrocystic change
Hormonal dysfunction as in fibrocystic changeSymptoms | Features |
Pain | Usually focal |
Firmness | Localized or diffuse with little cyclic variation |
Nodules | Firm or rubbery, smooth, moderately mobile, occasionally painful, not always palpable, depending on size and consistency of surrounding tissues |
|
|
|
 Simple cysts that are asymptomatic do not require treatment
Simple cysts that are asymptomatic do not require treatment If a solid mass or inspissated material is suspected in a patient with focal pain or nodularity: percutaneous aspiration first followed by core biopsy if aspiration is ineffective
If a solid mass or inspissated material is suspected in a patient with focal pain or nodularity: percutaneous aspiration first followed by core biopsy if aspiration is ineffective With mural proliferation or an intracystic tumor (papilloma or carcinoma): ultrasound-guided core biopsy with placement of marker clip or excisional biopsy
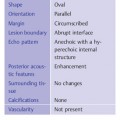
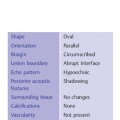
With mural proliferation or an intracystic tumor (papilloma or carcinoma): ultrasound-guided core biopsy with placement of marker clip or excisional biopsyShape | Oval or round |
Orientation | Parallel |
Margin | Circumscribed |
Lesion boundary | Abrupt interface |
Echo pattern | Anechoic |
Posterior acoustic features | Enhancement |
Surrounding tissue | No changes |
Calcifications | Occasionally present |
Vascularity | Not present* |
* Assessment of vascularity not indicated.
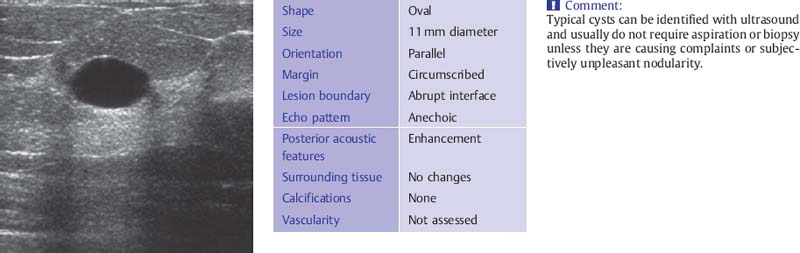
Fig. 7.1 Typical sonographic features of a cyst (13-MHz transducer).
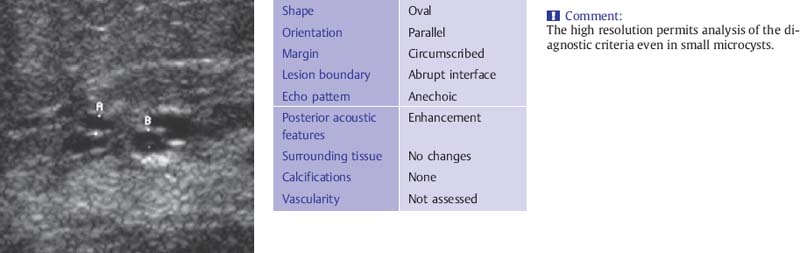
Fig. 7.2 Microcystic disease. Magnified view of a 20 × 20-mm area (13-MHz transducer) demonstrates a focal lesion composed of several microcysts, each 1–2mm in diameter.
Complicated Cysts
The diagnostic criteria for complicated cysts and complex cystic masses are summarized in Table 7.5.
Internal Echoes and Posterior Features
The high reflectivity of the anterior cyst wall often gives rise to reverberations (Figs. 7.6 a, b; 7.7 a, b), a band of echoes from the cyst wall that project into the interior of the cyst. These artifacts may be mistaken for solid areas of wall thickening. By moving the transducer and alternating compression and decompression, or by changing the angle of the transducer against the breast tissue or altering the patient’s position somewhat, the examiner can cause the reverberations to shift their position within the cyst and confirm them as artifacts. In addition, reverberations can be reduced by lowering the gain or power settings. Because the focal zone setting represents the highest concentration of acoustic energy, shifting the focal zone to a deeper level may also diminish the reverberations.
Cysts occasionally contain low-level internal echoes if the cyst fluid is inspissated, if the fluid contains hemosiderin, or if the cellularity of the fluid is increased (Fig. 7.8 a, b). This type of cyst, a complicated cyst in BI-RADS nomenclature, may resemble a fibroadenoma, especially when a transducer of 10 MHz or higher frequency is used. If doubt exists, cyst/solid differentiation can be accomplished by ultrasound-guided aspiration (Fig. 7.8 a, b). Despite their internal echoes, these cysts usually show an enhanced pattern of sound transmission. The cyst contents may also cause sound attenuation, producing a posterior acoustic shadow that creates the impression of a suspicious solid mass (Figs. 7.9 a, b; 7.10 a, b). This effect is common in cysts that contain milk of calcium and inflammatory cysts. The shadowing is most conspicuous when a high-frequency transducer is used.
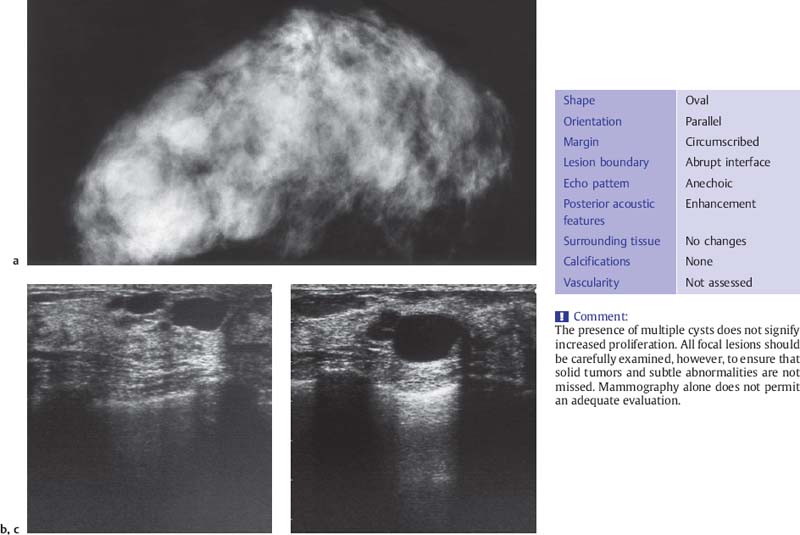
Fig. 7.3 a–c Macrocystic disease. a Mediolateral mammogram shows several rounded opacities in a dense breast. b, c Ultrasound reveals several macrocysts 4–20 mm in diameter (7.5-MHz transducer).
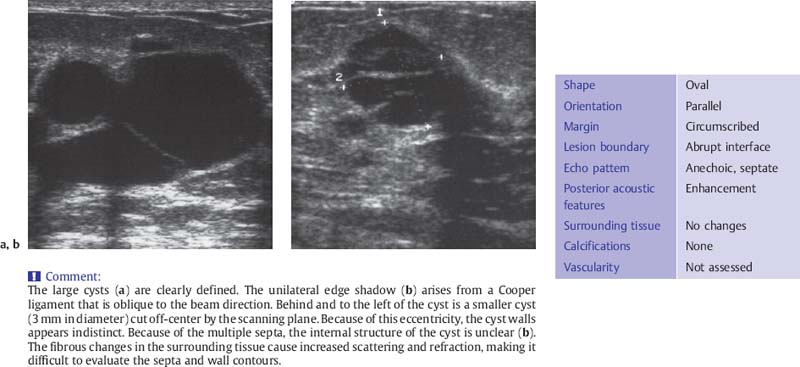
Fig. 7.4 a, b Cysts with multiple septations.
a Multiple septa within a cystic area 40 × 25 mm in size (7.5-MHz transducer).
b Two septa in a cyst measuring 16 × 17 mm.
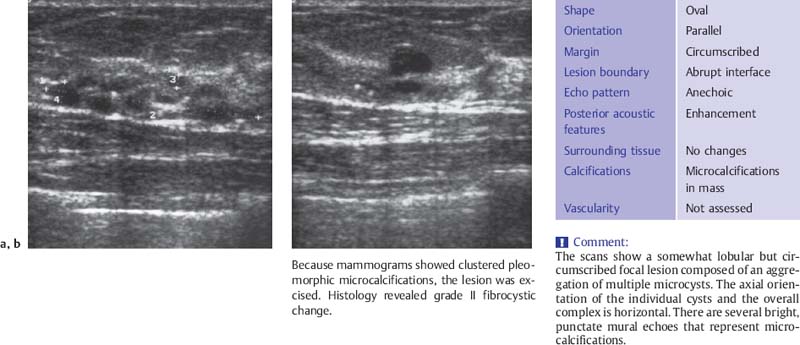
Fig. 7.5 a, b Microcystic lesions in a parenchymal area measuring 33 × 8mm in the sagittal plane. The area contains multiple micro-cysts 1–4 mm in diameter (10-MHz transducer). Because mammograms showed clustered pleomorphic microcalcifications, the lesion was excised. Histology revealed grade II fibrocystic change.
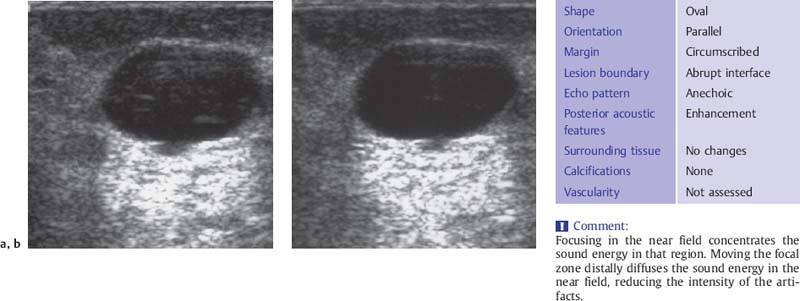
Fig. 7.6 a, b Intracystic reverberations. a Focus in the near field at 7 mm, b Focus shifted 5 mm deeper (10-MHz transducer).
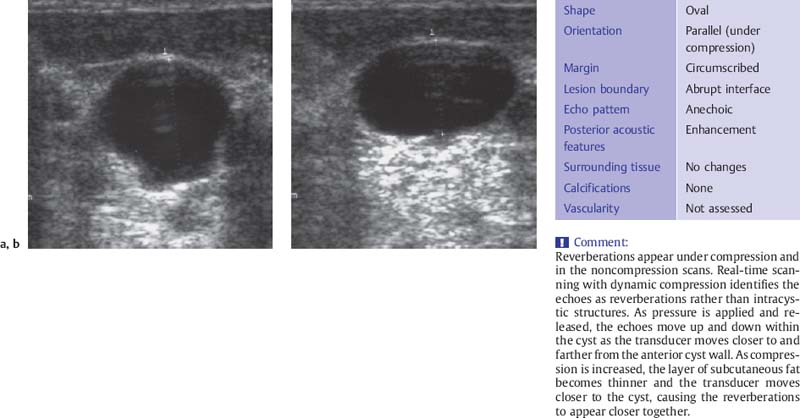
Fig. 7.7 a, b Intracystic reverberations.
a Without compression, anteroposterior diameter 15 mm.
b Light compression with the transducer, anteroposterior diameter 11 mm (10-MHz transducer).
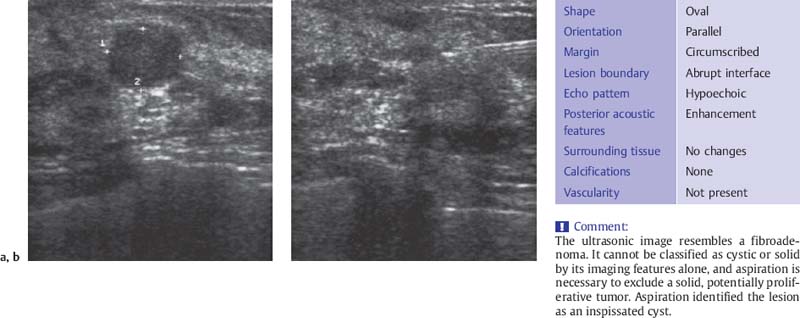
Fig. 7.8 a, b Echogenic cyst.
a Before aspiration.
b After aspiration, with the needle still in place (10-MHz transducer).
Aspiration can establish whether a lesion is cystic or solid and, in the case of a simple cyst, can avoid unnecessary surgery.
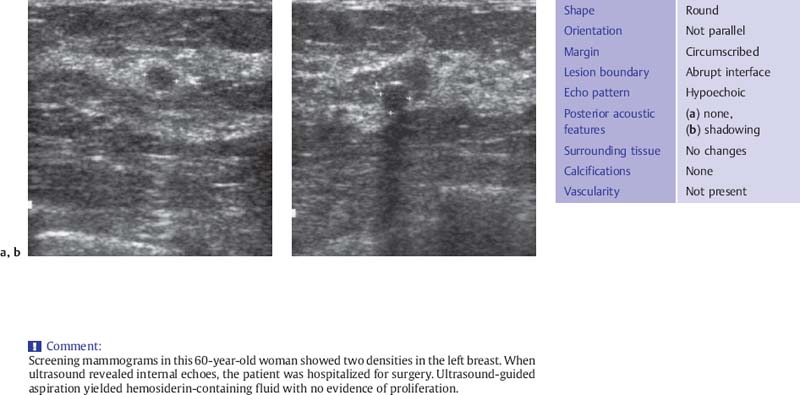
Fig. 7.9 a, b Hemosiderin-containing cyst.
a No shadowing or enhancement.
b Posterior acoustic shadow (10-MHz transducer).
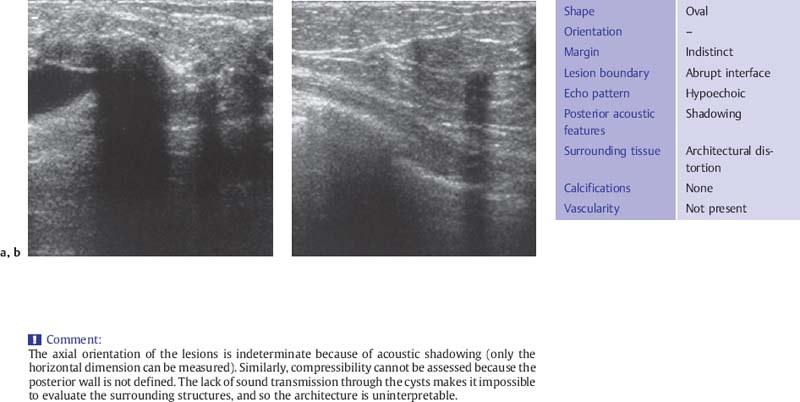
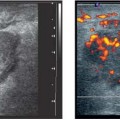
Fig. 7.10 a, b
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


