6 Degenerative and Demyelinating Diseases
Degenerative Diseases
Degenerative diseases of the brain (Tables 6.1, 6.2) are often referred for computed tomography (CT) scanning in patients undergoing evaluation for dementia. The most frequent cause of senile dementia is Alzheimer disease. The diagnosis of Alzheimer disease is based on specific clinical criteria, and cranial CT examination contributes to the diagnosis only by excluding other, potentially treatable causes such as intracranial masses (such as tumors or subdural hematoma) and normal-pressure hydrocephalus. This type of diagnosis is made with CT in approximately 1–2% of cases, depending on the patient selection. The percentage is higher in patients who have an immediate history of trauma, urinary incontinence, or gait disturbance.
| Type | CT features | |
|---|---|---|
| Cortical dementias | ||
• Alzheimer disease | Atrophy of temporal, parietal, and anterior frontal lobe cortices* | |
• Pick disease | Frontal and temporal cortical atrophy; the parietal and occipital lobes are relatively unaffected | |
| Subcortical dementias | ||
• Parkinson disease | The midbrain is essentially normal on CT. MRI shows significant narrowing of the pars compacta of the substantia nigra | |
• Parkinsonian syndromes | CT normal. MRI shows iron deposition in the putamen | |
• Huntington disease | Caudate atrophy (bicaudate ratio). The putamen and globus pallidus are less affected. Frontal and temporal atrophy | |
• Wilson disease | Ventricular dilatation, cortical atrophy, and decreased density of the basal ganglia | |
• Normal-pressure hydrocephalus | Ventricular dilatation disproportionate to the degree of sulcal enlargement | |
• Multiple sclerosis | Lesions in the periventricular white matter, cerebral atrophy | |
• HIV encephalopathy | Progressive diffuse leukoencephalopathy (symmetrical) | |
| Combined cortical and subcortical dementias | ||
• Vascular dementia | See p. 206 | |
– Multi-infarct dementia | ||
– Binswanger disease | ||
– Cerebral lacunae | ||
• Creutzfeldt-Jakob disease | Progressive, diffuse atrophy | |
• Hypoxic encephalopathy | Globus pallidus necrosis, with early hypodensities and calcifications in the late stage. Other basal ganglia may also be affected | |
HIV: human immunodeficiency virus.
* Distinguished from multi-infarct dementia, in which multiple infarcts of varying age are usually detected in both hemispheres.
| Disease | CT findings | MRI findings |
|---|---|---|
| Wilson disease | Generalized cerebral atrophy; rarely hypodensities in the caudate nucleus, lentiform nucleus, and thalamus | Increased T2-weighted signal intensity in caudate nucleus, lentiform nucleus, midbrain, and periaqueductal tissue; decreased T2-weighted signal intensity in the central putamen |
• MRI recommended | ||
| Huntington disease | Atrophy of the caudate nucleus, widening of the frontal horns, diffuse cerebral atrophy in the late stage | Like CT, T2-weighted MRI also shows hypointensity of these nuclei |
• MRI equivocal | ||
| Hallervorden-Spatz disease | Usually normal | High T2-weighted signal intensity in the pallidum, and low signal intensity in the globus pallidus |
| Leigh disease | Symmetrical hypodensities in the putamen and caudate nucleus, rarely in the pallidum or thalamus | Increased T1-weighted signal intensity, decreased T2-weighted signal intensity in these nuclei |
• MRI equivocal | ||
| Parkinson disease | Generalized cerebral atrophy | Generalized cerebral atrophy in multiple system atrophy (Parkinson plus), low T2-weighted signal intensity in the putamen |
• MRI recommended | ||
| Adrenoleukodystrophy | Bilateral hypodensity of the occipital white matter, advancing anteriorly; pseudogyral enhancement | Occipital-to-rostral progression of demyelination |
• MRI recommended | ||
| Alexander disease | Marked, diffuse white-matter hypodensity | White matter shows low Tl-weighted signal intensity, high T2-weighted signal intensity from rostral to occipital; pseudogyral enhancement |
• MRI recommended | ||
| Canavan disease | Diffuse white-matter hypodensity | White matter hypointense in T1-weighted image, hyperintense in T2-weighted image |
• MRI recommended | ||
| Pelizaeus-Merzbacher disease | Normal | White matter hypointense in T1-weighted image, hyperintense in T2-weighted image |
• MRI recommended | ||
| Cockayne syndrome | Atrophy and calcification of basal ganglia | Periventricular contrast reversal, sharply marginated lesions |
| Progressive multifocal leukoencephalopathy (PML) | Subcortical hypodensities, sharply marginated | Increased T2-weighted signal intensity (FLAIR sequence) corresponding to CT |
• MRI recommended | ||
| Progressive diffuse leukoencephalopathy (PDL) | Bilateral, predominantly frontal hypodensities sparing the subcortical white matter | Increased T2-weighted signal intensity (FLAIR sequence) corresponding to CT |
• MRI recommended |
The use of cranial CT in dementia patients depends on the diagnostic yield of treatable conditions, the patient’s and family’s need to know, and considerations of expense. As a rule, CT does not contribute to the differential diagnosis of dementias, beyond screening for potentially treatable causes.
Alzheimer Disease
Frequency: the most common form of dementia (6% prevalence after age 65); makes up approximately 60% of senile dementias.
Suggestive morphologic findings: CT can exclude multi-infarct dementia and other dementias. There are no specific CT features of Alzheimer disease, other than possible atrophy of the medial temporal lobe.
Procedure: Alzheimer disease is diagnosed clinically or by brain biopsy.
Other studies: functional imaging studies (nuclear medicine). Coronal magnetic resonance imaging (MRI) demonstrates changes in the medial temporal lobe.
Checklist for scan interpretation:
 Cerebral infarcts? White matter changes?
Cerebral infarcts? White matter changes?
 Other causes of dementia such as normal-pressure hydrocephalus, frontal tumors, etc.?
Other causes of dementia such as normal-pressure hydrocephalus, frontal tumors, etc.?
 Cortical atrophy? Accentuated in certain areas?
Cortical atrophy? Accentuated in certain areas?
 Pathogenesis
Pathogenesis
Alzheimer disease is the leading cause of dementia. Its prevalence increases with aging, starting at about 60 years of age, and it affects an estimated 6% of patients over the age of 65. It is believed to be caused by amyloid deposition in the neurons.
 Frequency
Frequency
Alzheimer’s type dementia is the most common form, accounting for 50–60% of cases.
 Histology
Histology
Histologically, there is a widespread loss of neurons that is manifested grossly by cerebral atrophy chiefly affecting the temporal lobes and hippocampus. The parietal lobes and anterior frontal lobes are also affected. Microscopic pathology consists of senile plaques in the gray matter and neurofibrillary tangles in the neurons. The diagnosis is confirmed by autopsy or brain biopsy.
 Clinical Manifestations
Clinical Manifestations
The early symptoms of the disease, which takes a progressive course, include personality changes and an inability to follow complex instructions or comprehend relationships. There is a progressive decline in cognitive functions. Memory impairment is very characteristic, but motor impairment is not an early feature. Other symptoms, such as loss of sphincter control, appear in later stages of the disease.
 CT Morphology
CT Morphology
The CT findings are nonspecific. Cortical atrophy predominantly affects the medial portion of the temporal lobe. The parietal and anterior frontal lobes are affected to a lesser degree.
Coronal T2-weighted MRI can demonstrate increased signal intensity of the hippocampus. Among the radionuclide imaging methods, positron-emission tomography (PET) findings are relatively characteristic, and consist of decreased uptake of 18F-deoxyglucose in the parietal lobes. Generally, this finding is bilateral and symmetrical.
 Differential Diagnosis
Differential Diagnosis
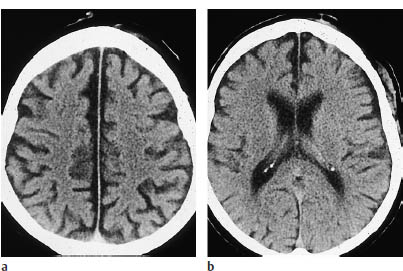
As noted above, the CT features of Alzheimer disease and other imaging findings are relatively nonspecific (Fig. 6.1). The best use of imaging procedures is to exclude less common but potentially treatable causes of senile or presenile dementia-most notably normal-pressure hydrocephalus, but also meningioma and other anterior fossa tumors. Pick disease has similar clinical features, but a different CT appearance (see below).
Pick Disease
Frequency: 10–30 times less common than Alzheimer disease.
Suggestive morphologic findings: marked atrophy of the frontal and temporal lobes, with normal-appearing parietal and occipital lobes.
Other studies: MRI demonstrates gliotic changes in the frontal and temporal cortex. Functional nuclear medicine studies show bilateral frontal hypoperfusion.
Checklist for scan interpretation:
 Other causes of dementia such as tumors or normal-pressure hydrocephalus?
Other causes of dementia such as tumors or normal-pressure hydrocephalus?
 Cortical sulci enlarged? Over which lobes?
Cortical sulci enlarged? Over which lobes?
 Pathogenesis
Pathogenesis
Pick disease is included with Alzheimer disease in the category of cortical dementias.
 Histology
Histology
Pick disease is characterized pathologically and radiologically by a focal atrophy affecting the frontal or temporal lobes. Microscopically, cytoplasmic inclusions (Pick bodies) are found in silver-stained sections from the affected cortex. The senile plaques and neurofibrillary tangles of Alzheimer disease, as well as other neuropathologic signs, are absent in Pick disease.
 Clinical Manifestations
Clinical Manifestations
Pick disease usually has an earlier clinical onset than Alzheimer disease, and initial changes often appear before age 65. Consistent with the morphologic findings, frontal lobe symptoms are common and consist of inappropriate social behavior (hyperorality, sexual disinhibition, etc.) and occasional depression or obsessive ideation.
 CT Morphology
CT Morphology
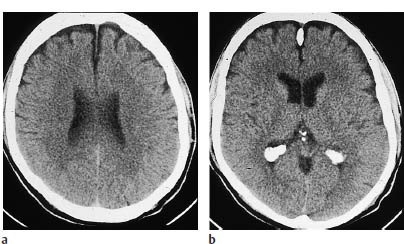
CT demonstrates focal cortical atrophy affecting the frontal lobes (Fig 6.2) or temporal lobes and sparing the parietal and occipital lobes. The precentral gyrus forms the “watershed” for cortical changes, with sulcal enlargement occurring anterior but not posterior to the gyrus.
 Differential Diagnosis
Differential Diagnosis
Pick disease should be considered in differential diagnosis whenever focal cortical atrophy is detected. Differentiation from Alzheimer disease is aided by the fact that atrophy of the caudate nucleus in Pick disease can lead to rounding of the frontal horns. Otherwise CT is used mainly to exclude other causes of dementia.
Creutzfeldt-Jakob Disease
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


