46 Degenerative Disk Disease I
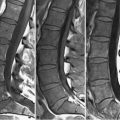
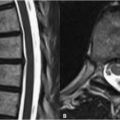
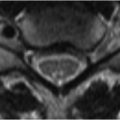
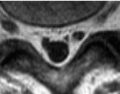
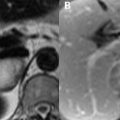
Techniques for the MRI evaluation of the lumbar spine differ from those implemented in the cervical and thoracic regions. For axial imaging in the cervical region, GRE T2W techniques are obtained due to potential problems from CSF pulsation and the small size of cervical spinal structures warranting thin slice imaging (2–3 mm). In distinction, slice thicknesses of 3 to 4 mm are acceptable in imaging of the lumbar spine where less prominent pulsation artifact also favors the acquisition of FSE T2WI. A thick coronal saturation slab is also routinely placed over the prevertebral tissues to eliminate artifacts from the aorta and vena cava, as well as abdominal motion. FSE has other advantages over GRE, including—due to its additional 180-degree refocusing pulse—diminished artifacts arising from differences in tissue susceptibility. Such artifacts play a role clinically, not only in postoperative patients wherein ferromagnetic implants may limit the diagnostic utility of GRE sequences, but also with respect to evaluation of spinal canal and neuroforaminal narrowing. With the latter, susceptibility effects from bone may exaggerate canal or foraminal narrowing depending upon the selection of imaging parameters. Tissue contrast with FSE T1WI of the lumbar spine is derived from differences in SI between high SI epidural fat versus the low SI thecal sac contents and intervertebral disk. This contrast is lost somewhat on FSE T2WI due to the preservation of hyperintense fat signal on such sequences.