Fig. 12.1
Dengue fever complicated by lung infection. Chest X-ray demonstrates slightly increased pulmonary markings in both lungs and patches and cords of shadows in the upper right lung (Note: The case and images were provided by Tang, YH. at Ruijin Hospital, Shanghai, China)
12.7.2 Dengue Hemorrhagic Fever and Severe Dengue Fever
In the cases of dengue hemorrhagic fever and severe dengue fever, pleural effusion is more common that occurs before or after the body temperature returns to normal. The quantity of effusion is positively proportional to the grading of dengue hemorrhagic fever. That is to say, the quantity of effusion in the cases of dengue hemorrhagic fever of grade III is larger than that in cases of dengue hemorrhagic fever of grades I and II. Thickened gallbladder wall is another common manifestation of dengue hemorrhagic fever that also occurs before or after the body temperature returns to normal. The thickness of the gallbladder wall exceeding 3 mm indicates edema (Fig. 12.2). In some cases, ascites can be found that is commonly located in the hepatorenal recess or in the space posterior to the urinary bladder. Nearly half of the cases with dengue hemorrhagic fever have concurrent pleural effusion and edema of the gallbladder wall. In the cases of dengue shock syndrome, pneumonia may occur, with imaging demonstrations of both lung consolidation and air bronchogram sign (Fig. 12.3). In addition, about 1/3 of the cases show splenomegaly (Fig. 12.4).
Case Study 2
A female patient aged 68 years was admitted due to mild edema of the bulbar conjunctiva and fine moist rales in the left lower lung. At day 4 after the onset, ecchymosis occurs at the site of injection.
Case Study 3
A female patient aged 23 years had complaints of fever for 5 days. Serological test revealed IgG and IgM antibodies against dengue fever. She was diagnosed with dengue fever. For more case detail and figures, please refer to, Addley HC, et al. 2011.

Fig. 12.2
Gallbladder lesions of severe dengue fever. (a) At day 3 after the onset, abdominal ultrasound demonstrates thickened gallbladder wall to about 6 mm. (b) At day 30 after the onset, reexamination by abdominal ultrasound demonstrates that the thickness of the gallbladder wall is about 3 mm (pointed by arrow) (Note: The case and images were provided by Guangzhou 8th People’s Hospital, Guangzhou, Guangdong, China
Case Study 4
A male patient aged 70 years had complaints of fever for 6 days. He then suffered from dyspnea, anemia, shock, and renal failure.
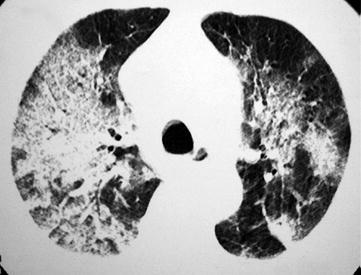
Fig. 12.3
Dengue hemorrhagic fever complicated by pneumonia. HRCT demonstrates large flakes of ground-glass opacities and consolidation shadows in both lungs and air bronchogram sign (Reprint with permission from Marchiori et al. Orphanet J Rare Dis, 2009, 5(4): 4)
Case Study 5
A case of dengue fever.
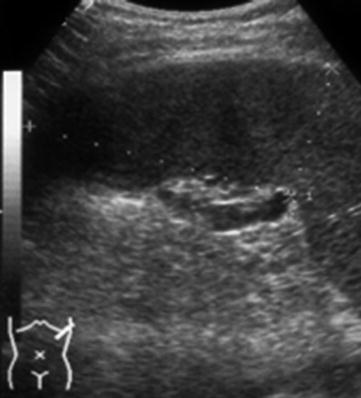
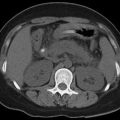
Fig. 12.4
Dengue fever. Abdominal ultrasound demonstrates splenomegaly (indicated by dotted line) (Reprint with permission from Wu KL, et al. Clin Ultrasound, 2004, 32(8): 386)
12.7.3 Dengue Fever with Encephalopathy
12.7.3.1 CT Scanning
Diffusive brain edema is common, and low-density lesions in the globus pallidus, hippocampal gyrus, thalamus, and internal capsule can also be found (Fig. 12.5). In some cases, pontine hemorrhage occurs. In rare cases, acute myelitis involving the cervical and thoracic spinal cord occurs. And in some cases, no abnormalities can be demonstrated.
12.7.3.2 MR Imaging
Diffusive brain edema is common, with multiple high-signal foci in the bilateral frontal lobes, paraventricles, pons, and cerebellum by T2WI and FLAIR. MR imaging demonstrates multiple hemorrhagic foci in the cases with intracranial hemorrhage, possibly complicated by encephaledema, cerebral infarction, and obstructive hydrocephalus (Figs. 12.6, 12.7, 12.8, and 12.9). The cases with the complication of acute myelitis are demonstrated to have multiple high-signal foci in the thoracic spinal cord (Fig. 12.10).
Case Study 6
A female patient aged 30 years had complaints of fever, projectile vomiting, convulsion, and drowsiness.
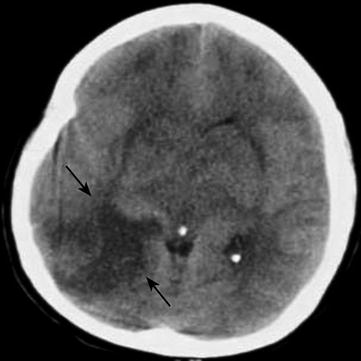
Fig. 12.5
Dengue fever complicated by encephalitis. CT scanning demonstrates flakes of low-density lesions in the right occipital lobe and temporal lobe, with quite clearly defined boundaries (pointed by arrow)
Case Study 7
A female patient aged 25 years had occurrence of fever, vomiting, and drowsiness after the onset of the disease.
Fig. 12.6




Dengue fever complicated by encephalitis. (a) CT scanning demonstrates multiple irregular low-density lesions in the bilateral frontal lobes, occipital lobes, and temporal lobes, with clearly defined boundaries (pointed by arrow). (b) Coronal MR imaging and FLAIR demonstrate multiple symmetric round-like foci in high signals in the bilateral temporal lobes (pointed by arrow). (c) Sagittal contrast MR imaging demonstrates enhancement of meninges (pointed by arrow)
Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
