Bowing may be congenital or acquired. The direction of bowing of the tibia may suggest the etiology. Anterolateral bowing of the tibia is associated with neurofibromatosis, tibial fractures, and congenital pseudarthrosis of the tibia. Posteromedial tibial bowing is an isolated finding not associated with other conditions.
Table 5.57 Diaphysis: bowing
Diagnosis
Findings
Comments
Physiologic bowling of toddlers
Femur and tibia are mildly bowed.
Predilection for the first 2 y of life. Corrected within 6 mo of walking. Reaches adult pattern of mild valgus by 6–7 y.
Plastic/bowing fracture
Bowing of radius or ulna are the most common sites.
If the radius is fractured, the accompanying bone (ulna) may be fractured (and vice versa).
Widening of the medial aspect of the growth plate in older children with an ossified distal femoral epiphysis. The weight-bearing part is always the widest.
Recurrent fracture with malposition
Bowing of fragile bones after repeated fractures.
Occurs in all bone disorders with increased bone fragility (e.g., osteogenesis imperfecta and other intrinsic sclerotic bone dysplasias).
Changes in the posteromedial proximal tibial epiphysis that lead to growth suppression. Any varus angulation at the knee in children > 2 y is considered abnormal.
Pseudarthrosis of the tibia
Anterolateral bowing.
Almost always unilateral. Associated with neurofibromatosis (40%–50% of pseudarthroses of the tibia).
Osteogenesis imperfecta, achondroplasia, and camp-omelic dysplasia, for example.
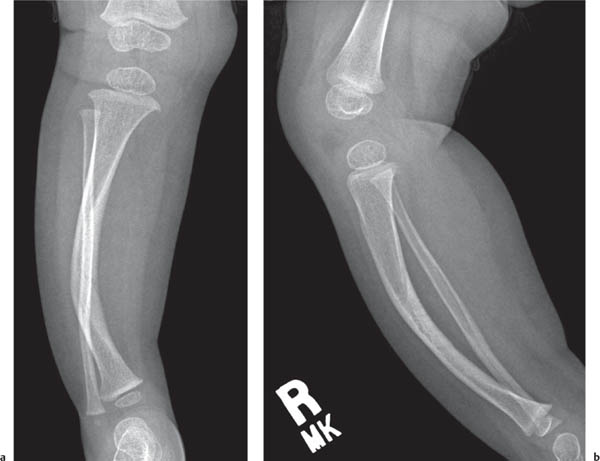
Fig. 5.90 Rickets. Hypophosphatemic rickets and bowing of both femurs.Fig. 5.91a, b Fibrous dysplasia with ground-glass matrix producing anterolateral bowing of the tibia.Fig. 5.92a, b Neurofibromatosis with anterolateral bowing of the tibia.Fig. 5.93 Unknown congenital syndrome with congenitally bowed femurs and dislocated hips.Fig. 5.94 Osteogenesis imperfecta with a bowed left femur and a contralateral fracture.Fig. 5.95a, b Osteogenesis imperfecta. Anteromedial bowing of the tibia in a 4-year-old with osteogenesis imperfecta.
Only gold members can continue reading. Log In or Register to continue