Abstract
Diffuse fine nodules are the expected presentation of intravascular dissemination of tuberculosis, which is a life-threatening complication. Perception of the fine nodular opacities is often difficult and may require high resolution CT of the chest for confirmation. Because the tuberculous organisms are in the blood vessels of the lung, sputum cultures may not be positive and biopsy may be required to confirm the diagnosis. Tuberculosis must be distinguished from a number of fungal infections and rarely bacterial or viral infections. Silicosis and coal worker’s pneumoconiosis may produce fine nodular opacities, but the nodules often have an upper lobe distribution and are more variable in size than the nodules of miliary tuberculosis. Small nodular metastases are also more variable in size than miliary tuberculosis.
Keywords
coal worker’s pneumoconiosis, histoplasmosis, metastases, miliary tuberculosis, sarcoidosis, silicosis
Questions
- 1.
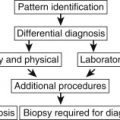
Based on the radiologic appearance of the case illustrated in Fig. 17.1 , which one of the following diagnoses is the most urgent one?
- a.
Miliary tuberculosis.
- b.
Silicosis.
- c.
Langerhans cell histiocytosis.
- d.
Hypersensitivity pneumonitis.
- e.
Sarcoidosis.

Fig. 17.1
- a.
- 2.
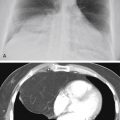
Regarding Fig. 17.2 , which of the following is the most likely diagnosis?
- a.
Sarcoidosis.
- b.
Metastatic carcinoma.
- c.
Langerhans cell histiocytosis.
- d.
Hypersensitivity pneumonitis.
- e.
Histoplasmosis.

Fig. 17.2
- a.
Mark the following questions True or False:
- 3.
____Sarcoidosis and silicosis may present with the pattern seen in Fig. 17.1 in combination with hilar adenopathy.
- 4.
____Bronchoscopy with biopsy is contraindicated in the evaluation of patients in whom the pattern is believed to be secondary to tuberculosis.
Discussion
Detection of very small nodules is a serious challenge for the radiologist. Nodules measuring 1 to 3 mm (see Fig. 17.1 ) are marginally detectable on the chest radiograph and may require high-resolution computed tomography (HRCT) for confirmation ( Fig. 17.3, A and B ). Examination of gross specimens often reveals many more nodules of a much smaller size than can be resolved as separate opacities on the chest radiograph. Heitzman suggested that miliary nodules are probably seen on the radiograph because of the effect of summation—that is, a “stacked coin effect.” 235 These very small nodules are sometimes more easily appreciated on the posteroanterior view in the costophrenic angle and on the lateral view in the retrosternal clear space. Furthermore, small nodular opacities may occasionally be confused with very small pulmonary vessels seen on end. This mistake is usually avoided by identifying an associated, branching vascular pattern around the nodule. Also, miliary nodules are typically much more diffuse than the fine nodular appearance created by normal vessels.

The sharpness of the borders of the nodules is an important criterion for narrowing the differential. Small opacities may be caused by small, sharply defined interstitial nodules or by minimal involvement of the distal air spaces, which results in ill-defined opacities with an acinar pattern. 175 , 601 This distinction is the key to limiting the differential. If the pattern includes small, fluffy, or ill-defined opacities, then alveolar edema, exudate, or hemorrhage should be considered. The presence of ill-defined borders should prompt examination of the radiograph for other signs of air space filling disease (see Chapter 15 ). In contrast, the pattern of very small but sharply defined or discrete opacities should reassure the radiologist that the nodules are more likely interstitial and are thus associated with one of the entities listed in Chart 17.1 .
- I.
Infections
- A.
- B.
Fungus infections (histoplasmosis, 97 blastomycosis, 450 , 561 coccidioidomycosis 373 ), Aspergillosis (rare), 46 cryptococcosis (rare) 200 , 252 , 321
- C.
Bacterial infections (bronchopneumonia—unusual early presentation), nocardiosis 208
- D.
- A.
- II.
Environmental diseases
- A.
Silicosis and coal workers’ pneumoconiosis 80 , 86 , 429
- B.
- C.
- D.
Hypersensitivity pneumonitis or allergic alveolitis (farmer’s lung) 353 , 497 , 570
- E.
Hard metal pneumoconiosis 299
- A.
- III.
Langerhans cell histiocytosis 1 , 585
- III.
- VIII.
Metastatic tumor 175
- A.
Thyroid carcinoma
- B.
Melanoma 76
- C.
Other adenocarcinomas (e.g., gastrointestinal tumors)
- A.
- IX.
Other
- A.
Alveolar microlithiasis (rare) 467
- B.
Gaucher disease 645
- C.
Granulomatosis with polyangiitis (rare)
- D.
Immunotherapy (bacillus Calmette-Guérin) 272
- A.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


