Clinical Presentation
The patient is a 76-year-old man who complains of neck and base of neck pain as well as debilitating headaches that awaken him at night. He also complains of shoulder pain with any overhead activity. The patient has noted some moderate swallowing difficulty over the last several years.
Imaging Presentation
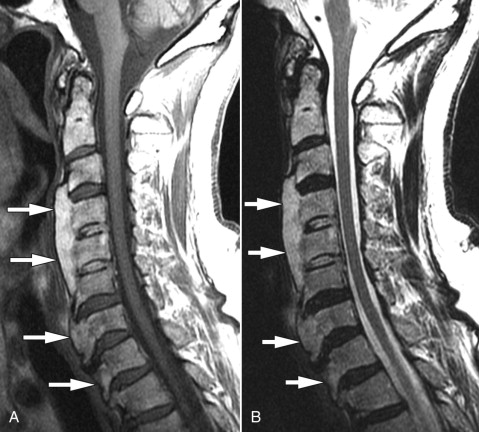
Sagittal T1- and T2-weighted magnetic resonance (MR) images demonstrate flowing bone signal intensity along the ventral vertebral bodies from C3-T1. There are no degenerative changes of the intervertebral discs. The findings represent diffuse idiopathic skeletal hyperostosis (DISH). The signal intensity of this finding suggests that the regions of DISH may have gained a marrow cavity ( Fig. 20-1 ) .
Discussion
In 1950, Forestier and Rotes-Querol described a process that was characterized by flowing spinal osteophytes and stiffness and termed it senile ankylosing hyperostosis . During the next several years, many different names were given to the same condition including Forestier disease , generalized juxtaarticular ossification of the vertebral ligaments, and spondylosis hyperostotica . In 1975, Resnick further classified this process and termed it diffuse idiopathic skeletal hyperostosis (DISH) .
DISH is a common disease. It is most commonly seen in people over the age of 50. Studies have reported that 28% of people with an average age of 65 have DISH. Other studies show a prevalence of DISH in 15% of women and 25% of men over the age of 50, and 26% in women and 28% in men over the age of 80.
People may present with nonspecific back pain or stiffness. Dysphagia can be a complication of DISH secondary to large anterior osteophytes. Many patients are asymptomatic, with DISH being discovered incidentally.
The thoracic spine is the typical location of DISH, followed by the lumbar spine and then the cervical spine. When it occurs in the cervical spine, it often involves the lower segments. When it occurs in the lumbar spine, it often involves the upper segments. In the thoracic region, the anterior osteophytosis is predominantly right sided. It is thought that there is a protective effect from aortic pulsation on the left side of the spine. Patients with DISH and situs inversus show ossification mainly on the left side of the thoracic spine. The syndesmophytes of DISH project horizontally from the vertebral body and have the appearance of flowing candle wax.
DISH can have extraspinal manifestations, including enthesophytes involving the iliac wing, tendinous ossification of the knee, hyperostosis of any bone in the foot, calcaneal spurs, calcification of the Achilles tendon, osseous excrescences in the shoulder, spurs of the olecranon and hyperostosis, and spur formation in the hand and wrist.
Imaging Features
DISH is predominantly a radiographic diagnosis. Forestier demonstrated the initial manifestations that were refined by Resnick and Niwayama. The first of the criteria is to have flowing ossification along the anterolateral aspect of at least four contiguous vertebra. Secondly, there is preservation of disc height in the involved segment with a relative absence of degenerative changes. Lastly, there is absence of zygapophyseal ankylosis or sacroiliac degeneration. Plain radiography is the most cost-effective imaging study and may be all that is necessary to diagnose DISH. Contiguous anterior osteophytes are readily discerned with relative preservation of the disc spaces and absent/minimal facet joint degenerative changes ( Fig. 20-2 ) . Computerized tomography (CT) with sagittal reformatted images can demonstrate the same findings as plain radiography ( Fig. 20-3 ) . With CT, one is also able to visualize the effect the ossification has on the adjacent soft tissues. Magnetic resonance imaging (MRI) is not necessary for the diagnosis of DISH.