Renal failure may be classified as prerenal when secondary to a reduction in the renal perfusion pressure gradient, renal when the result of intrinsic disease of the renal parenchyma, and postrenal when secondary to an abnormality of urine outflow.
Prerenal renal failure may arise from alterations in renal artery perfusion or venous drainage. Renal artery stenosis results in decreased perfusion. Renal vein thrombosis results in increased backpressure and edema. Postrenal causes of abnormal renal function are typically those causing obstruction to the urine outflow from calculi, ureteropelvic dysfunction, or masses.
Renal parenchymal abnormalities may be divided into those that involve the entire kidney, such as rejection, glomerulonephritides, amyloidosis, and drugs, and those that are either primarily cortical or primarily medullary, such as nephrocalcinosis. These conditions are discussed in this section.
Imaging Overview
Glomerulonephritis (GN) has no specific imaging findings. Pathologic and immunologic assessment of biopsy samples continues to be the mainstay in diagnosis. Ultrasound evaluation of the kidneys is useful to exclude other causes of renal function impairment. Ultrasonography also may demonstrate calculi and nephrocalcinosis. The kidneys may be enlarged in acute GN or may be small in chronic GN. Morphologically the kidneys show a smooth contour. Excretory or intravenous pyelography (IVP) (requires the administration of potentially nephrotoxic iodinated contrast and is therefore generally not performed in patients with diffuse renal parenchymal disease. Noncontrast computed tomography (CT) is useful for visualizing stones and the distribution of nephrocalcinosis. Contrast-enhanced CT, as with IVP, requires nephrotoxic iodinated contrast and therefore is typically not used if renal function is abnormal. Magnetic resonance imaging (MRI) is insensitive to urinary stones and nephrocalcinosis, but it is useful in the imaging of renovascular abnormalities. Newer techniques such as diffusion- and perfusion-weighted imaging and ultrasmall superparamagnetic iron oxide (USPIO)-enhanced imaging may have advantages when evaluating diffuse renal diseases by not requiring a biopsy.
Radiography
Intravenous urography may show bilaterally smooth, enlarged or small kidneys. The kidneys may show poor contrast excretion, depending on the stage of renal failure. Apparent expansion of the renal sinus fat is a commonly seen secondary sign of diffuse atrophy due to chronic renal diseases ( Figure 64-1 ).

Ultrasonography
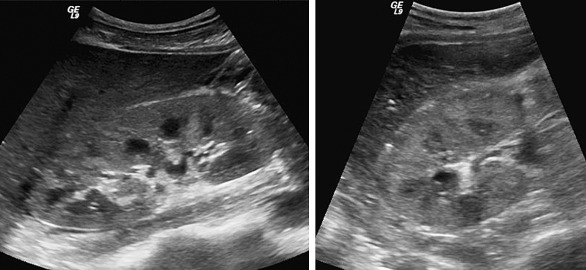
Renal echogenicity is typically equal to or less than that of the adjacent liver or spleen, respectively. Corticomedullary differentiation is normally better visualized on the right than the left. Abnormal ultrasonographic findings include increased renal echogenicity and bilateral enlarged kidneys ( Figure 64-2 ). The utility of ultrasonography is to evaluate for hydronephrosis and vascular abnormalities (inflow or outflow) as causes for renal failure. The absence of both suggests intrinsic renal parenchymal disease. In chronic GN, the kidneys may show increased echogenicity and are usually small or show cortical loss with smooth margins. There may be proliferation of sinus fat.
Doppler ultrasonography, although nonspecific, can assist in the differential diagnosis of acute renal failure. The normal renal resistive index is between 0.6 and 0.7. The RI is elevated in a large number of conditions, including prerenal, parenchymal, and postrenal causes. These include hepatorenal syndrome, renal vasculitis, acute crescentic and proliferative GN, and tubulointerstitial disease. Thus, without prior knowledge of the diagnosis, an elevation is useful only to suggest that renal parenchyma is indeed abnormal. The RI is normal in acute primary or secondary GN. Renal Doppler imaging has been used to follow treatment response.
Computed Tomography
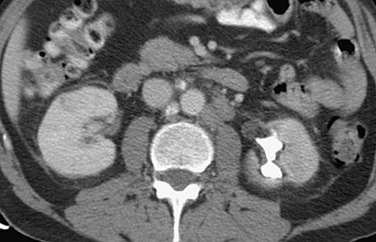
Noncontrast CT may show cortical calcification in chronic GN. The kidneys appear small and have a smooth contour in chronic GN but may show scarring in chronic pyelonephritis ( Figure 64-3 ). CT scan may show normal or bilateral renal enlargement in acute GN ( Figure 64-4 ).

Magnetic Resonance Imaging
Nonspecific changes in renal size ( Figure 64-5 ) and enhancement are seen in diffuse renal disease. Recent literature suggests that USPIO-enhanced MRI may be useful. USPIO-enhanced imaging shows the distribution of macrophages. Diffuse macrophage infiltration in rejection versus focal medullary in acute tubular necrosis (ATN), monitoring of drug reactions in immunosuppressed patients, and differentiating between reversible and chronic abnormalities are potential future uses of this modality.

Nuclear Medicine
Renal function can be assessed using technetium-99m ( 99m Tc)-labeled mercaptoacetyl triglycine ( 99m Tc-MAG3) or diethylenetetraminepentaacetic acid ( 99m Tc-DTPA). Cortical agents such as dimercaptosuccinic acid (DMSA) are used for evaluation of scars, such as in patients with pyelonephritis. Captopril renography is useful in evaluation of renal vascular diseases.
Imaging Algorithm
The first step is to assess for dilation of the pelvicalyceal system and ureter with ultrasonography to determine if renal failure is renal or postrenal ( Figure 64-6 ). If there is no hydronephrosis, Doppler imaging may be performed to assess for renovascular disease.
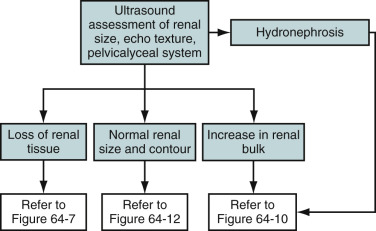
Renal size should be assessed in all patients. Renal size varies considerably within populations and by gender from 10 to 14 cm in males and 9 to 13 cm in females. Disease processes may initially cause an increase in renal size as a result of acute-phase edema and then cause a chronic decrease in renal size as a result of fibrosis. Thus, prior or serial ultrasound evaluation may be of greater benefit than a single measurement. The finding of small kidneys therefore implies that chronic diffuse renal disease is present.
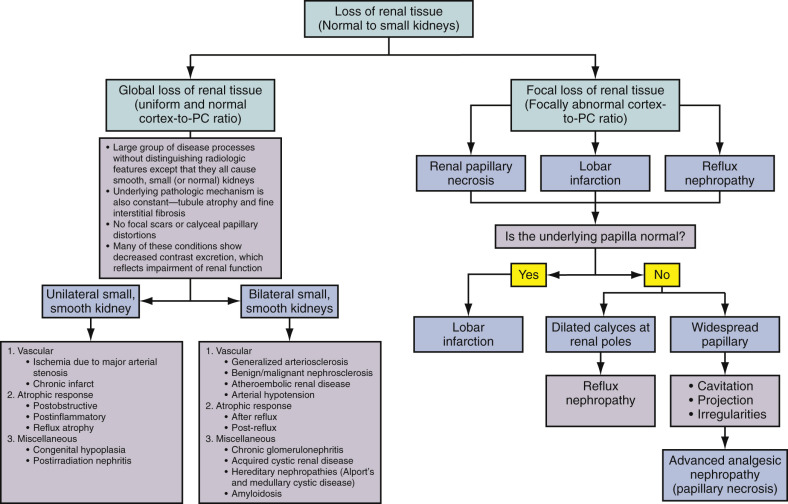
Diseases that manifest as small kidneys are further categorized into those with smooth or irregular contour ( Figure 64-7 ). Contour irregularity is seen with renal infarction, reflux nephropathy, and advanced analgesic nephropathy. Of these, only renal infarction will not cause any underlying calyceal abnormality ( Figure 64-8 ). Smoothly marginated, small kidneys are seen in diseases that cause tubular atrophy and fine interstitial fibrosis. No focal scars or calyceal papillary distortions are noted. Further differentiation is limited in this subgroup except determination if the process is unilateral or bilateral (see Figure 64-7 ). Diseases that cause renal cortical atrophy also may result in compensatory renal sinus lipomatosis with little alteration in bipolar renal length ( Figure 64-9 ).

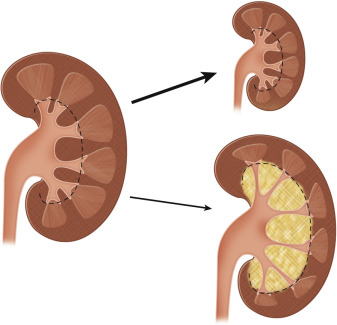
The conditions that cause nephromegaly may do so in a focal or diffuse manner ( Figure 64-10 ). Focal renal masses are most commonly secondary to cysts or neoplasms and rarely may be a focal manifestation of a disease that is usually diffuse (e.g., focal nephritis).
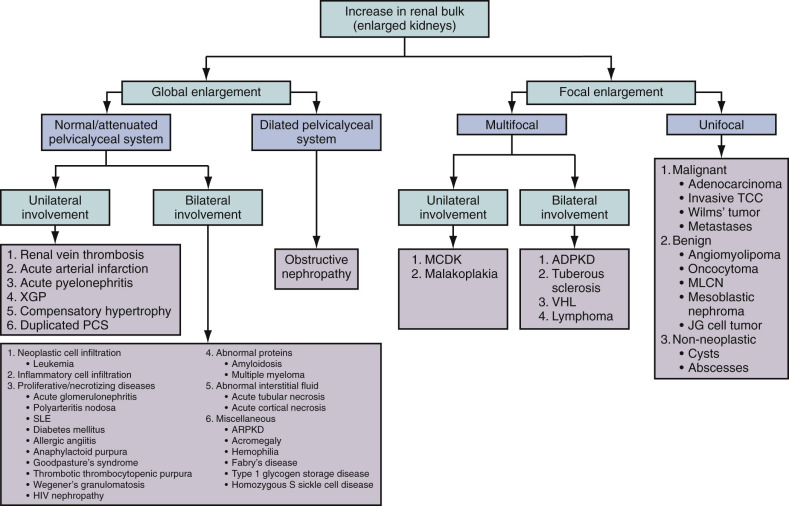
Unilateral diffuse nephromegaly may be secondary to renal edema from renal vein thrombosis or urinary obstruction. Diffuse unilateral nephromegaly also may be seen when physiologic compensatory hypertrophy occurs in the setting of contralateral renal failure. The causes of bilateral renal enlargement include infiltrative processes and infectious and immune disorders, most of which consist of glomerular diseases (see Figure 64-10 ). The spectrum of changes in renal size, contour, and pelvicalyceal system is summarized in ( Figure 64-11 ).

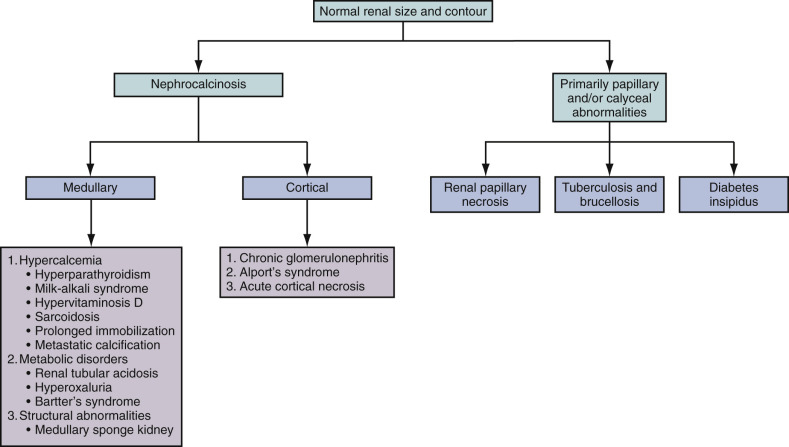
Several diffuse parenchymal diseases do not cause any change in renal size ( Figure 64-12 ). This group consists of diseases causing nephrocalcinosis and those that present primarily with calyceal or papillary abnormalities. Included in this latter subset are essentially all causes of renal papillary necrosis as well as granulomatous infections such as tuberculosis (TB) and brucellosis (see Figure 64-12 ).
Differential Diagnosis
The differential diagnosis of diffuse renal parenchymal diseases includes the following:
- •
Immunoglobulin A (IgA) disease (Berger’s nephropathy) is the most common type of GN in adults worldwide.
- •
Henoch-Schönlein purpura is a systemic variant of IgA nephropathy that causes vasculitis of small vessels of which GN is a feature.
- •
Postinfectious GN occurs after streptococcal infection (usually of the skin), after a latency of 10 to 14 days. It manifests as nephritic syndrome, with a positive antistreptolysin O titer as diagnostic, and recovery is the rule in 2 to 3 weeks.
- •
Mesangiocapillary GN can be primary or secondary to systemic lupus erythematosus, viral hepatitis, or hypocomplementemia; it usually manifests as a nephrotic syndrome but can be nephritic, with inevitable progression to end-stage renal failure.
- •
Rapidly progressive GN (crescentic GN) has a poor prognosis, with rapid progression to kidney failure over weeks. Vasculitic disorders such as Wegener’s granulomatosis, polyarteritis, and Goodpasture’s syndrome are diseases manifesting solely as rapidly progressive GN. Patients with Wegener’s granulomatosis and Goodpasture’s syndrome may have hemoptysis in addition to renal failure.
- •
Minimal change GN causes 80% of nephrotic syndrome in children but only 20% in adults.
- •
Focal segmental glomerulosclerosis (FSGS) may be primary or secondary to reflux nephropathy, Alport’s syndrome, heroin use, or human immunodeficiency virus (HIV) infection. FSGS presents as a nephrotic syndrome with varying degrees of renal impairment; 50% of people with FSGS progress to renal failure.
- •
Membranous GN is the leading cause of nephrotic syndrome in adults (35%). It is usually idiopathic but may be associated with cancers (lung, bowel), infection (hepatitis, malaria), drugs (penicillamine), and systemic lupus erythematosus. A third of patients have stable disease, and a third progress to end-stage kidney failure.
Differential Diagnosis
The differential diagnosis of diffuse renal parenchymal diseases includes the following:
- •
Immunoglobulin A (IgA) disease (Berger’s nephropathy) is the most common type of GN in adults worldwide.
- •
Henoch-Schönlein purpura is a systemic variant of IgA nephropathy that causes vasculitis of small vessels of which GN is a feature.
- •
Postinfectious GN occurs after streptococcal infection (usually of the skin), after a latency of 10 to 14 days. It manifests as nephritic syndrome, with a positive antistreptolysin O titer as diagnostic, and recovery is the rule in 2 to 3 weeks.
- •
Mesangiocapillary GN can be primary or secondary to systemic lupus erythematosus, viral hepatitis, or hypocomplementemia; it usually manifests as a nephrotic syndrome but can be nephritic, with inevitable progression to end-stage renal failure.
- •
Rapidly progressive GN (crescentic GN) has a poor prognosis, with rapid progression to kidney failure over weeks. Vasculitic disorders such as Wegener’s granulomatosis, polyarteritis, and Goodpasture’s syndrome are diseases manifesting solely as rapidly progressive GN. Patients with Wegener’s granulomatosis and Goodpasture’s syndrome may have hemoptysis in addition to renal failure.
- •
Minimal change GN causes 80% of nephrotic syndrome in children but only 20% in adults.
- •
Focal segmental glomerulosclerosis (FSGS) may be primary or secondary to reflux nephropathy, Alport’s syndrome, heroin use, or human immunodeficiency virus (HIV) infection. FSGS presents as a nephrotic syndrome with varying degrees of renal impairment; 50% of people with FSGS progress to renal failure.
- •
Membranous GN is the leading cause of nephrotic syndrome in adults (35%). It is usually idiopathic but may be associated with cancers (lung, bowel), infection (hepatitis, malaria), drugs (penicillamine), and systemic lupus erythematosus. A third of patients have stable disease, and a third progress to end-stage kidney failure.
Glomerulonephritis
Etiology
GN is a complex spectrum of immune-mediated renal disease characterized by inflammation of the glomeruli that may be divided into primary and secondary types. Primary GN is intrinsic to the kidney without additional systemic manifestations. Most cases are immune mediated. The most common type is poststreptococcal GN (PSGN). Secondary GN is associated with systemic disease, including certain infections (bacterial, viral, or parasitic pathogens), drugs, systemic disorders (systemic lupus erythematosus, vasculitis), or cancers.
Prevalence and Epidemiology
Acute Glomerulonephritis
Acute GN comprises 25% to 30% of all cases of end-stage renal disease (ESRD) in the United States. Approximately one fourth of affected patients present with acute nephritis. Internationally, PSGN is associated with pharyngeal infection rather than cutaneous infection. Acute GN has no predilection for any racial or ethnic group. Poor socioeconomic status is associated with an increased risk for PSGN. There is a 2 : 1 male-to-female ratio. Acute GN can occur at any age. Acute postinfectious GN usually develops in children 6 to 10 years of age but can affect any age group.
Chronic Glomerulonephritis
In the United States, chronic GN is the third leading cause of ESRD and accounts for 10% of patients on dialysis. A recent decline in chronic GN in these countries has been noted, with an increase in diabetic nephropathy in patients on dialysis. ESRD and death are common outcomes unless renal replacement therapy is instituted.
Clinical Presentation
Patients may present with isolated hematuria, may be asymptomatic, may have nephrotic and nephritic syndromes, or may have either acute or chronic renal failure. Acute GN develops over days and manifests as proteinuria, hematuria, hypertension, edema, and oliguria. Rapidly progressive GN develops over weeks to months, and chronic GN develops over months to years.
Pathology
Kidneys are grossly normal or enlarged in diseases that manifest acutely and those without significant fibrosis and small and scarred in chronic disease and those with renal fibrosis. There may be hypercellularity with thickening of the glomerular basement membrane, hyalinization with deposition of amorphous proteinaceous material, and sclerosis that leads to obliteration of the glomerular tuft.
Pyelonephritis
Etiology
Acute pyelonephritis is an infection of the renal parenchyma and renal pelvis inclusive of the tubules and interstitium commonly with a gram-negative organism such as Escherichia coli (>80%), Proteus, Klebsiella, or Enterobacter. Fungi or mycobacteria also may be causative. Inflammatory changes in the glomerulus (GN) are often excluded. Most cases are ascending infections from the lower urinary tract ( Figure 64-13 ), and a few are hematogeneous.
Emphysematous pyelonephritis is a necrotizing infection of the renal parenchyma seen primarily in diabetic patients. Xanthogranulomatous pyelonephritis (XGP) is usually secondary to chronic renal obstruction, as may be seen with ureteropelvic junction syndrome, congenital abnormalities, tumor, stricture, or stones in the calyces or renal pelvis. These patients often have comorbid conditions such as diabetes, pregnancy, systemic disease, or chronic liver disease.
Prevalence and Epidemiology
Pyelonephritis may be divided into uncomplicated and complicated subgroups. Uncomplicated pyelonephritis refers to cases in which there are no permanent sequelae. Complicated pyelonephritis is associated with recurrent disease, structural abnormalities, diabetes, pregnancy, immunosuppression, and prolonged symptoms (>2 weeks in duration).
Predisposing factors for pyelonephritis include urinary tract obstruction, vesicoureteral reflux, pregnancy, urinary tract instrumentation, preexisting renal disease or systemic predisposition such as diabetes mellitus, and immunosuppression.
Acute pyelonephritis implies an acute infection of the renal parenchyma, commonly infectious in cause. It is more common in adults than in children, in females younger than the 40 years of age, and in males older than the age of 65 years. A subtype of uncomplicated acute pyelonephritis affects young women.
Chronic pyelonephritis is renal injury induced by recurrent or persistent renal infections characterized by progressive renal scarring that may lead to ESRD. It is most commonly seen in children owing to the much higher incidence of vesicoureteral reflux in this population. It is more common in females.
Emphysematous pyelonephritis is a life-threatening, fulminant, necrotizing upper urinary tract infection (UTI) associated with gas in the kidney. A rare infection, it affects adults of any age (mean, age 54 years). It is two to six times more common in females than in males and is often seen in diabetic patients.
XGP is an unusual form of chronic pyelonephritis in which there is a chronic suppurative granulomatous infection of the kidney and surrounding tissues. An abnormal host response leads to destruction and replacement of the renal parenchyma by lipid-laden macrophages. XGP is typically a diffuse condition; however, a rare focal form may be seen in children. It can occur at any age but is more common between ages 45 and 65 years. Women are three times more commonly affected than men. Proteus and E. coli are the most common causative organisms.
The presentation of pyelonephritis in the pediatric age group is different from that in the adult and may be challenging to the clinician. There is less easy differentiation between upper and lower UTI on physical examination and by laboratory methods. Imaging is therefore of greater consideration even in the presence of uncomplicated disease or single episodes. The American Academy of Pediatrics recommends that children with confirmed UTI should undergo ultrasound of the kidneys and bladder. However, voiding urethrocystogram should not be performed routinely after the first febrile UTI.
Clinical Presentation
Patients present with fever, malaise, dysuria, flank pain, and tenderness. Laboratory data may show an elevated erythrocyte sedimentation rate, increased white blood cell count, and proteinuria. Children may show failure to thrive.
XGP may mimic a neoplasm, with patients presenting with anorexia, a palpable mass, or weight loss. A fistulous tract to the skin may be noticed if there is involvement of surrounding tissues. Emphysematous pyelonephritis may manifest as a crepitant mass, a very suggestive finding. The laboratory studies may show hyperglycemia, acidosis, electrolyte imbalance, and thrombocytopenia. Blood, urine, or aspirate may be positive on culture.
Pathology
In acute pyelonephritis, microabscesses are seen on the renal surfaces, mostly on the poles. These are often referred to as polar abscesses. Microscopic examination shows interstitial or tubular necrosis and mononuclear cell infiltrate with fibrosis. Chronic pyelonephritis appears as a small shrunken kidney with scars and blunted calyces. Emphysematous pyelonephritis is evident as a suppurative necrotizing infection of the renal parenchyma and perirenal tissues with multiple cortical abscesses. The gross appearance of XGP is a mass of yellow tissue with regional necrosis and hemorrhage, superficially resembling that of a renal cell carcinoma. The pathognomonic microscopic feature is the lipid-laden “foamy” macrophage accompanied by both chronic- and acute-phase inflammatory cells. Focal abscesses may be observed.
Imaging
Acute Pyelonephritis
Acute pyelonephritis is usually multifocal. The diagnosis is commonly a clinical one based on increased renal size. American College of Radiology appropriateness criteria state that “imaging adds little to management if the patient responds to therapy within 72 hours” for uncomplicated pyelonephritis. As a result, imaging studies are rarely indicated for the diagnosis of acute uncomplicated pyelonephritis in the adult who presents with typical signs and symptoms. Imaging may be warranted if the presentation is atypical or confusing or if the patient’s condition deteriorates or does not respond to therapy.
The imaging modality of choice is contrast-enhanced helical and/or spiral CT when there is suspicion of the development of a complication of acute pyelonephritis, in both adults and children. The algorithmic approach for the imaging diagnosis of acute pyelonephritis is summarized in Figure 64-14 .
Contrast-enhanced CT is the imaging study of choice in adults. It is more sensitive than ultrasonography or excretory urography and can more readily identify alterations in renal parenchymal perfusion, alterations in contrast excretion, presence of perinephric fluid, and nonrenal disease. Classically, a striated nephrogram may be seen ( Figure 64-15 ).
Ultrasonography can sometimes detect acute pyelonephritis, but a negative study does not exclude the possibility.
Imaging may be required to make the diagnosis in infants and children in whom pyelonephritis manifests insidiously. The American Academy of Pediatrics recommends ultrasonography and either voiding cystourethrography or radionuclide cystography in the 2-month to 2-year age group after a single episode of pyelonephritis.
Renal cortical scintigraphy with 99m Tc-DMSA or glucoheptonate is primarily used to identify the presence of scars rather than acute infection, because both may manifest as photopenic areas. Scintigraphy is more sensitive for scarring than ultrasonography. Both scar and acute pyelonephritis show focal areas of diminished uptake in approximately 90% of patients ( Figure 64-16 ). Vesicoureteral reflux is an important cause of pyelonephritis in children and can be detected and quantified with radionuclide cystography.
Imaging studies in conjunction with urologic procedures, including cystoscopy and excretory urography, may be used during follow-up examination to evaluate for urinary tract abnormalities that can predispose the patient to infection.
Chronic Pyelonephritis
Chronic pyelonephritis is associated with major anatomic abnormalities, urinary tract obstruction, renal calculi, renal dysplasia, or vesicoureteral reflux in young children. Recurrent or chronic infections are often present historically. The disease may be focal, segmental, or diffuse and unilateral or bilateral. Typically there is a scarred contracted kidney. There also may be focal atrophy (usually upper pole). A patient may present with a unilateral small contracted kidney and contralateral compensatory hypertrophy.
CT is the imaging modality of choice to help diagnose chronic pyelonephritis. It can show cortical scarring with distribution that could be focal, multifocal, and diffuse and involve one or both kidneys ( Figure 64-17 ) and also compensatory contralateral renal hypertrophy. Radioisotopic scanning with 99m Tc-DMSA is more sensitive than excretory urography for detecting renal scars. This is the preferred test in patients in the pediatric age group because it is sensitive and easy to perform and requires less radiation ( Figures 64-18 and 64-19 ).
Emphysematous Pyelonephritis
Emphysematous pyelonephritis is unilateral more often than bilateral, and the left side is more often involved than the right side. On radiography, air can sometimes be seen overlying the renal fossa ( Figure 64-20 ). Findings of excretory urography include increased renal size and delayed or absent excretion. CT helps differentiate between air in parenchyma and air and fluid collections ( Figure 64-21 ). On ultrasound, there may be shadowing, ring-down artifacts, and nonvisualization of the kidney ( Figure 64-22 ).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


