31 Disk Herniations
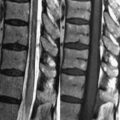
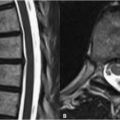
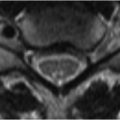
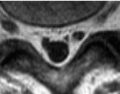
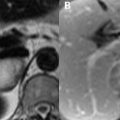
Disk herniations (i.e., focal disk protrusions) in the cervical spine occur most frequently between the 4th and 7th vertebral bodies due to the greater mobility of the spinal column in this region. Optimal imaging technique is essential for detection of these and other cervical spine abnormalities, as the structures being evaluated are small and artifacts related to gross patient motion are common. Motion artifact (i.e., swallowing) is frequent, but correctable with saturation pulses or through changes in the direction of the phase encoding gradient. CSF pulsation artifact may be reduced by gradient moment nulling and cardiac gating. The small size of intervertebral disks warrants selection of a slice thickness of 3 mm or less, and for this reason imaging at 3 T—where a 3-mm slice thickness is standard—is imperative. Routinely acquired sequences for the evaluation of cervical disk herniations include sagittal and axial T1, sagittal FSE T2, and axial GRE T2WI. Whereas in the lumbar spine T1WI may detect the displacement of high SI epidural fat, indicating the presence of herniation, the lack of such fat in the cervical region renders this pulse sequence less useful. On FSE T2WI a herniated disk may mimic the low SI appearance of an osteophyte. Thus, (axial) GRE T2WI is the preferred sequence for evaluation of cervical disk herniations. GRE lacks the refocusing pulses present in spin and fast spin echo sequences and is thus more sensitive to T2* (magnetic susceptibility) effects. The high SI of the fluid-filled disk is thus well seen against the calcium-rich bone, which exhibits a very low SI.