Introduction
Medical use of radiation has increased during the past decade and currently is estimated to account for approximately 50% of the radiation exposure to the U.S. population, with computed tomographic (CT) examinations accounting for the majority of this exposure. The harm from radiation during diagnostic imaging studies is related primarily to the risk for cancer induction, which conservatively is determined using a nonthreshold linear relationship, such that the risk increases linearly with the radiation exposure. Determination of this risk takes into account the amount and type of radiation, age at exposure, total exposure, gender of the person, and organs that are exposed.
Acceptable image quality requires a certain amount of radiation exposure to the patient during multidetector computed tomographic (MDCT) examinations to ensure adequate signal-to-noise ratio (SNR) needed for confident diagnostic interpretation. MDCT imaging parameters can be adjusted depending on the specific indication of the study and body habitus of the patient to optimize image quality and reduce radiation dose exposure. In this chapter we discuss current techniques available to reduce radiation dose during MDCT body imaging.
Issues Pertinent to Radiation Dose for Multidetector Computed Tomography Studies
Radiation dose reduction must be performed within the context of maintenance of adequate image quality. When performing MDCT examinations the parameters of the examination should be chosen based on the type of the scanner, the size of the patient, anatomic region of interest, and the clinical question(s) to be answered. Parameters of the MDCT scanner that affect radiation include scanner geometry, tube current, tube voltage, scanning modes, scan length, collimation, table speed, gantry rotation time, and filters. Because of differences in scanners, including detector configuration and quantity of output of the x-ray beam, migration of protocols from one scanner to another often requires changing protocol parameters. Understanding the specifics of the scanner allows for appropriate selection of parameters to minimize radiation exposure while maintaining image quality.
Variations in body size and density will attenuate the x-ray beam differently. As a generalization, more radiation is needed to penetrate larger patients as a result of scatter of the primary beam from a larger body size. Although increases in tube current may be necessary in imaging obese patients, it has been shown that this modification does not increase the absorbed dose for internal organs. In certain anatomic locations such as the pelvis, there is increased attenuation of the x-ray beam by the surrounding bones and higher amounts of radiation are needed in this region to maintain image quality comparable to that in the thorax. Additionally, imaging in anatomic locations that have intrinsically low contrast-to-noise ratios, such as the pelvis, require a higher SNR than in other anatomic locations, such as the chest.
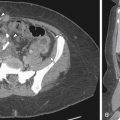
The clinical question for which the scan is being performed needs to be considered in regard to the reconstruction algorithm, z-axis coverage, and the necessary SNR, all of which will determine the overall radiation exposure and parameter settings for the CT examination. For example, imaging of the abdomen and pelvis for renal calculi can be done with an overall lower radiation dose than for appendicitis imaging because of the intrinsically high contrast-to-noise ratio present between a small renal stone and the surrounding ureter ( Figure 4-1 ).

Strategies for Dose Reduction
The parameters of the CT examination can be altered in isolation; however, for effective dose reduction and maintenance of image quality, maximal effect will be achieved if the parameters are evaluated in relation to each other.
Tube Current
Current MDCT tubes can generate outputs up to 800 mA. A constant milliampere can be applied for evaluation of the abdomen and pelvis; however, software advances now allow for the milliampere to vary during the study while maintaining a constant noise level; this results in lower radiation exposure to the patient in the range of 20% to 35% for body imaging. This application, known as automatic tube current modulation (ATCM), can be performed in several manners depending on the individual CT scanner being used. Angular dose modulation occurs in the X and Y plane, reducing the milliampere in the anterior and posterior projections while maintaining a higher tube current along the lateral projection (compared with the anterior and posterior projections), which contributes more to the image noise; this reduction in dose is usually based on the previous 180 to 360 degrees of scanning. Modulation of dose can also occur along the z-axis of the patient, this type of modulation is based on the scout film and has the ability to reduce dose in anatomic areas of the body that attenuate the beam the least, such as the chest compared with the abdomen ( Figure 4-2 ). A combination of these two techniques is also available on many scanners.

ATCM software uses several input parameters for appropriate application. A user input value that describes the type of desired image quality (noise index, reference image acquisition, reference tube–current time product value, or reference standard deviation) is required. This value can vary depending on the body habitus, the indication of the study, and the reconstruction algorithm. Appropriate orientation of the patient with respect to the gantry is necessary for ATCM to work effectively. Miscentering the patient within the scanner can change the distance between the patient and the x-ray beam resulting in either magnification or minification of the scout film. This misrepresentation of the body can result in an inappropriate increase or decrease in the milliampere settings. The relationship of the beam to the patient also will change such that the beam will no longer be centered on the patient; rather, it may be located more anteriorly or posteriorly, resulting in a change to the absorbed dose to the more superficially located organs.
Tube Energy
The options on the CT scanner for the tube energy setting are more limited than those of milliampere, ranging from 80 to 140 kVp. Historically a setting of 140 kVp was used for routine clinical examinations to preserve tube life and to allow for optimal penetration of a wide variety of body sizes. Recent work has demonstrated that for a smaller body habitus, a reduced peak kilovoltage can be used on a routine basis to reduce radiation exposure while maintaining adequate image quality. Additionally, when administering intravenous contrast, reducing the peak kilovoltage will not only lower the overall radiation exposure but also can improve the image quality because imaging is performed closer to the k-edge of iodine (33 kV). This has shown to be of particular benefit when performing dedicated MDCT angiograms.
Z-Axis Coverage
Reducing the z-axis coverage will linearly decrease the overall radiation exposure to the patient. For abdominal and pelvis imaging this is of considerable importance because imaging caudal to the pubic symphysis and cranial to the diaphragms has been shown to have minimal change in patient outcomes while increasing radiation exposure to patients. Increasing the z-axis coverage above the diaphragms contributes to greater radiation exposure to the breasts, and this has been noted to be of particular concern for young female patients.
Scan Time
The acquisition time for a CT examination will vary depending on z-axis coverage (discussed previously), rotation time, pitch, and beam collimation (width). A faster gantry rotation time will decrease radiation exposure to the patient if all other parameters are held constant and may also result in fewer motion artifacts. Increasing the pitch can result in a lower radiation dose. This can lead, however, to generation of helical artifacts and reduction in SNR. Decreasing the pitch will increase the radiation dose; however, this is often needed for MDCT angiograms, for which interslice gaps need to be minimized.
Using a larger beam collimation (width) will increase the z-axis coverage per rotation. Because of the penumbra effect, a small portion of the x-ray beam is used during helical scanning to maintain consistent image quality to all detectors (known as overbeaming); the contribution of overbeaming to total radiation exposure can be minimized by using a wide beam width and/or higher pitch. Depending on the configuration of the scanner, wider beam widths may require using wider length detectors (i.e., scanning at 1.25 vs. 0.625 mm), which may limit one to a larger slice thickness width.
Filters
Filtration of the x-ray beam can allow for removal of photons that do not add to image quality but contribute to a patient’s radiation exposure. Bowtie filters shape the x-ray beam, and when matched to the field of view, the scatter of the beam outside the field of view is reduced. This has been shown to reduce the amount of radiation on the surface of the body. Bismuth shields placed on the patient lower energy photons that do not add to image quality but increase radiation exposure to the patient. These have been shown to be of particular use in reducing the radiation filter dose to superficial organs such as the breast, thyroid, and eyes.
Postprocessing filters can also be applied to improve image quality and their use with lower radiation dose acquisition is unclear.
Reconstruction Algorithms
The prescribed reconstruction algorithm will determine how much noise is acceptable for the examination. Although current scanners can acquire isotropic data sets, more frequently data sets are viewed in reconstructed 3- to 5-mm-thick images. Thicker reconstructed data sets can accommodate more noise without degrading the image quality. For example, when a thick reconstruction algorithm is used (i.e., 5- vs. 1.25-mm-thick images), a lower radiation dose technique can be used (4×) to maintain a similar image quality. Care should be taken, however, with this approach because partial volume averaging effects will be amplified. Currently, iterative reconstruction techniques are being investigated as an alternative mode of data reconstruction to filter back projection techniques to reduce radiation exposure during MDCT examinations.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


