CHAPTER 17
Double-Outlet Right Ventricle and Double-Outlet Left Ventricle
Definition
Double-Outlet Right Ventricle
Double-outlet right ventricle (DORV) refers to a spectrum of cardiac lesions unified by an abnormal ventriculoarterial connection.1 DORV is most commonly defined as a condition in which more than 50% of both the aortic root and the pulmonary artery arise from the ventricle with right morphological features.2–5 A ventricular septal defect (VSD) is usually, but not always, present.5
DORV was first described in 1703.6 It was considered to be one type of transposition of the great arteries (TGA). In 1898, Vierordt referred to DORV as a partial transposition because only the aorta was actually transposed as the pulmonary artery originates appropriately from the right ventricle.7
In 1949, Taussig and Bing8 described a patient with “complete transposition of the aorta and levoposition of the pulmonary artery.” They described the first reported case in which both great arteries arose from the right ventricle, but the VSD was related to the pulmonary artery and not the aorta, as had been the case in all previous reports.5 In 1952, Braun et al9 described a case in which “the right ventricle serves as a double outlet ventricle.” They classified it as a partial transposition of the Fallot type.
The term “double-outlet right ventricle” was first used by Witham10 in 1957. He considered it to be a partial transposition complex in which both great arteries arose from the right ventricle. He divided his cases of DORV into two groups—the Fallot type and the Eisenmenger type—depending on whether pulmonary stenosis was present or absent.7
A classification system for DORV was first developed by Neufeld et al11,12 in 1961. They separated cases into those with and those without pulmonary stenosis and included an additional category for those with “other intracardiac malformations.” They later subcategorized the group without pulmonary stenosis on the basis of the position of the VSD in relation to the crista supraventricularis and the great arteries.13
In 1972, Lev et al14 classified DORV on the basis of the relationship of the VSD to the two great arteries, including subaortic, subpulmonary, doubly committed (involving both great vessels), or noncommitted (distant from either great artery). They advocated expanding the definition of DORV to include cases in which only two cusps and part of a third cusp of both semilunar valves originate from the right ventricle. Additionally, they considered the Taussig-Bing type of DORV as a spectrum ranging from cases in which both great arteries arise wholly from the right ventricle to those with pulmonary-mitral continuity, as in complete transposition.
In 1982, Van Praagh developed the most widely accepted classification of DORV, which included the following2,5,15–21:
• DORV with a subpulmonary VSD
• DORV with a doubly committed (both subaortic and subpulmonic) VSD
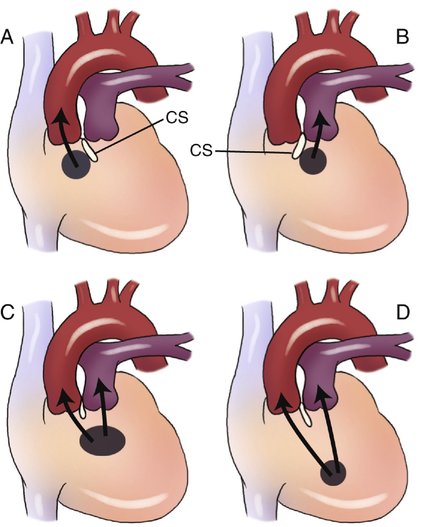
• DORV with a remote VSD (noncommitted) (Fig. 17–1)
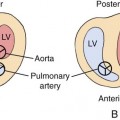
Four types of great artery relationships at the level of the semilunar valves have been described in DORV19:
• Aorta right and posterior to the pulmonary artery (normal)
• Aorta right and lateral to the pulmonary artery (side by side)
• Aorta right and anterior to the pulmonary artery (dextromalposition)
• Aorta left and anterior to the pulmonary artery (levomalposition)
In 1978, Sridaromont et al20 evaluated angiographically 72 patients with proven DORV to determine the location of a VSD when it was associated with various great artery relationships. They identified 16 possible combinations (Fig. 17–2).
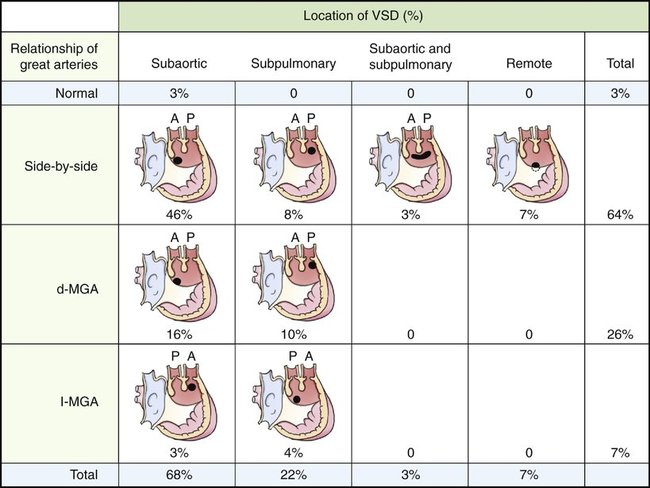
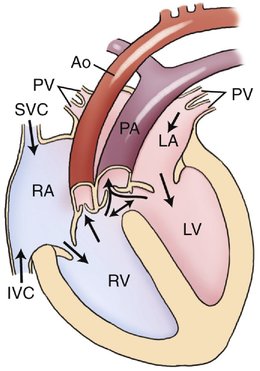
The combination of a subpulmonary VSD with side-by-side great vessels was found in 8% of patients. This type of DORV is commonly considered the classic Taussig-Bing heart (Fig. 17–3).14 Pulmonary stenosis is not associated with this particular anomaly; therefore, the pulmonary artery is usually dilated. Anatomically, a subpulmonary VSD is usually located in a more anterior position than is a subaortic VSD.
Remote or noncommitted VSDs were identified in 7% of patients in this series. Similar to the doubly committed VSD, all were associated with side-by-side great vessels. The most common form recognized as a remote VSD is a complete atrioventricular canal defect with DORV.7 This type can, however, be located in the anterior, middle, or posterior muscular septum.22 DORV with a remote VSD is often associated with the heterotaxy syndromes. In a more recent study, Bradley et al21 reviewed 393 cases of DORV. They also reported DORV with a subaortic VSD as being the most common form, occurring in 47% of cases. DORV with a noncommitted VSD was found in 26%, DORV with a subpulmonic VSD was found in 23%, and DORV with a doubly committed VSD was diagnosed in 4%.
DORV with an intact ventricular septum has also been reported.20,23–26 It is, however, exceedingly rare. This type of DORV is usually associated with hypoplasia of the left ventricle and with anomalies of the mitral valve.
Although the Van Praagh system is still considered by many to be the traditional classification of DORV, many authors thought that it was not ideal because it is based solely on the anatomical relationship between the VSD and the great arteries and does not consider the surgical approach. In 2000, the Society of Thoracic Surgeons and the European Association of Cardiothoracic Surgery adopted four types of DORV on the basis of clinical presentation and treatment27:
• VSD-type: DORV with subaortic VSD
• Fallot-type: DORV with subaortic or double committed VSD and pulmonary outflow stenosis
• TGA-type (Taussig-Bing): DORV with a subpulmonary VSD
Double-Outlet Left Ventricle
Double-outlet left ventricle (DOLV) is far less common than DORV. It is defined as a malformation in which the aorta and the pulmonary artery both arise exclusively or predominantly from the ventricle with left morphological features.28 Early reports of DOLV by Fragoyannis and Kardalinos29 in 1962 and by Ruttenberg et al30 in 1964 described the origin of both great arteries from the left ventricle, but these appeared to represent instances of a double-outlet ventricle with right ventricular morphological features with atrioventricular discordance. This sparked controversy as to the actual existence of DOLV. In 1970, however, Paul et al31 reported the first autopsy proven case of DOLV with an intact ventricular septum. Van Praagh et al32 published a review of 109 cases of DOLV in 1988, in which they described 26 different types.
Their classification was based on three primary criteria:
• The situs of the atria, the ventricles, and the great arteries: Normal situs (solitus), situs inversus, and situs ambiguous have all been reported.33–37
• The alignment or commitment of the atria, the ventricles, and the great vessels: Alignment can be concordant, discordant, double-inlet, or absent right or left atrioventricular connection.
• Location of the VSD or other associated cardiovascular anomalies
As in DORV, four basic anatomic locations of VSDs have been associated with DOLV32:
In the Van Praagh series, three main types of DOLV were observed. The most common type was DOLV with a subaortic VSD, which was observed in 48% of all cases and in 73% of cases with situs solitus and atrioventricular concordance (n = 71). This group of patients was further categorized on the basis of the great artery relationships (right anterior or left anterior aorta) and the presence or absence of aortic or pulmonary stenosis.32
The most common form of DOLV with a subaortic VSD had a right anterior or right lateral aorta (35 of 71 patients). Of these 35, 29 patients (83%) also had subvalvular and valvular pulmonary stenosis. This type of DOLV is also referred to as the tetralogy type of DOLV because it is often confused clinically and angiographically with tetralogy of Fallot as a result of the associated pulmonary stenosis.28 The remaining six patients with a right anterior aorta and DOLV with subaortic VSD, but without pulmonary stenosis, were reported to have clinical and angiographic characteristics similar to complete transposition (dextrotransposition) of the great vessels.
The great vessel orientation and clinical findings of the two entities are similar, with the degree of aortic override and commitment to the morphological left ventricle being the only clearly distinguishing feature.28
Embryology
Historically, DORV was thought to result from a failure of the normal spiraling of the aorta and pulmonary trunk, resulting in abnormal positioning. However, more recent research confirms that the primitive right ventricle is in fact a DORV, containing the conotruncus. If migration of the aortic side of the conotruncus toward the mitral valve is incomplete, the DORV anatomy persists.38 Another refinement of accepted embryology suggests that DOLV is actually caused by the misalignment and arrest of the ventricular septum.39
Occurrence Rate
DORV is considered a rare congenital malformation, occurring in approximately 0.033 to 0.09 per 1000 live births.40–43 The frequency among abortuses and stillborn infants is reported to be 2.4%.44 There does not appear to be an ethnic or a sex predilection in DORV.



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


