Key Points
- •
Providers must readily recognize the five main discriminating artifacts produced by lung ultrasound: lung sliding, A-lines, B-lines, consolidation, and effusion.
- •
The presence or absence of discrete artifacts allows for an accurate, algorithmic approach in determining the causes of dyspnea and respiratory failure.
- •
Clinical application of lung ultrasound findings is an essential skill for providers using point-of-care ultrasound.
Background
Physical examination and chest radiography have limited accuracy when trying to determine the etiology of dyspnea or acute respiratory failure. Ultrasound of the thorax has proven to be a more accurate bedside tool that can rapidly detect the presence or absence of pulmonary pathology, including interstitial syndrome, pleural effusion, pneumothorax (PTX), and consolidation. The systematic use of thoracic ultrasound to evaluate respiratory failure has significant potential to facilitate diagnosis and management of acutely ill patients.
General Principles
An approach to thoracic ultrasound in the clinical evaluation of patients has been previously described in the BLUE protocol (see Chapter 8 ). Systematically compiling lung ultrasound findings at these points allows for rapid identification of possible etiologies in acute dyspnea or respiratory failure. Following is an adapted algorithm that may be used for interpreting patterns found during a systematic thoracic ultrasound exam in the context of acute respiratory failure, remembering to always interpret ultrasound findings in the clinical context ( Figure 38.1 ).
Step 1: Is there lung sliding?
- 1.
If yes, proceed to Step 2.
- 2.
If no—Look for absent lung pulse or presence of stratosphere sign on M-mode. If found, look for lung point to diagnose PTX. If no lung point found, consider confirmatory test with chest x-ray or CT scan to rule out PTX.
- 1.
Step 2: What is the underlying pattern at the pleural surface?
- 1.
A-line pattern—Perform a DVT study
- a.
Positive for DVT: Pulmonary embolism
- b.
Negative for DVT: Chronic obstructive pulmonary disease (COPD)/asthma most likely; consider metabolic or neurologic causes of respiratory failure
- a.
- 2.
B-line pattern—Characterize B-line pattern
- a.
Bilateral and uniformly distributed without areas of sparing along with a smooth, thin pleural line: Pulmonary edema
- b.
Unilateral, patchy pattern with irregularly thickened pleura or diminished sliding: Early or atypical pneumonia
- c.
Bilateral with areas of sparing and irregularly thickened pleura: Acute respiratory distress syndrome (ARDS)
- a.
- 3.
Effusion—Consider as primary cause if size is large enough to induce dyspnea
- 4.
Consolidation—Characterize consolidation
- a.
Volume loss with either no air bronchograms or static air bronchograms —Atelectasis
- b.
Dynamic air bronchograms, normal or expanded lung volume, no lung flapping/sinusoid sign—Pneumonia
- a.
- 1.

The following four case scenarios demonstrate the integration of an algorithmic approach using thoracic ultrasound in the evaluation of patients with acute respiratory failure.
Case Studies
Case Presentation
The rapid-response team was called to evaluate a patient in respiratory distress on the telemetry unit. The patient was a 76-year-old woman with a history of diabetes mellitus and hypertension. She was admitted a week prior to the cardiac care unit with a non-ST elevation myocardial infarction and congestive heart failure. She was stabilized there and then underwent a cardiac catheterization with stents placed in the right coronary and left circumflex arteries. Left ventricular ejection fraction was estimated at 35%.
Vital signs: T 37° C, Pulse 120 (telemetry demonstrated atrial fibrillation), Blood pressure 103/55, Respiratory rate 34, Oxygen saturation 92% with non-rebreather mask. Physical exam: The patient was in moderate respiratory distress. Heart sounds were tachycardic and irregular and jugular venous distention was evident. Lungs sounds were rapid and shallow with scattered rhonchi at the bases. The extremities had 1+ bilateral pitting edema.
Assessment
The differential diagnosis for this patient included pulmonary edema, pulmonary embolism, cardiac tamponade, and pneumonia. The history and physical exam of this patient, including jugular venous distension, could be consistent with pulmonary edema, yet chest auscultation has limited sensitivity for this diagnosis. An S3 can be difficult to detect. Although chest radiography could be helpful, lung ultrasound can be performed more rapidly and with greater diagnostic accuracy.
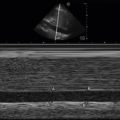
BLUE points of the anterior hemithoraces reveal the presence of lung sliding bilaterally with A-line patterns ( Figures 38.2 and 38.3 and ![]()
![]() ). A rapid assessment for deep vein thrombosis identified a noncompressible right common femoral vein ( Figure 38.4 and ).
). A rapid assessment for deep vein thrombosis identified a noncompressible right common femoral vein ( Figure 38.4 and ).



Case Resolution
Absence of a B-line pattern on ultrasound provided evidence that clinically significant pulmonary edema was not present. Thus, other etiologies for respiratory distress were sought. The A-line pattern increased the probability that the patient was suffering from an etiology of respiratory failure that did not affect the pleural interface viewed by ultrasound, namely pulmonary embolism, obstructive pulmonary disease (COPD or asthma), metabolic, or neurologic disorders. The finding of a proximal lower extremity deep vein thrombosis supported the diagnosis of pulmonary embolism. The patient was given IV fluids and a bolus of heparin followed by a continuous infusion. Aggressive diuresis was avoided based on the ultrasound findings.
Case Pearl
Venous branch points are common sites to find a deep vein thrombus. Close examination at the junction of the common femoral vein with the greater saphenous vein and the trifurcation of the popliteal vein can reveal the remnant of a larger deep vein thrombosis that separated and migrated to the lungs causing pulmonary embolism.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


