, Ahmad Ameri1 and Mona Malekzadeh2
(1)
Department of Clinical Oncology, Imam Hossein Educational Hospital, Shahid Beheshti University of Medical Sciences (SBMU), Shahid Madani Street, Tehran, Iran
(2)
Department of Radiotherapy and Oncology, Shohadaye Tajrish Educational Hospital Shahid Beheshti University of Medical Sciences (SBMU), Tehran, Iran
The acute ear complications of radiation therapy include external, middle, and inner ear injuries. The acute external ear complications include otitis externa or skin reactions involving the preauricular region, the auricle, and the external auditory canal that occur in about 28% of head and neck cancer patients treated with radiation therapy [1]. The acute middle ear complications that include mastoiditis, Eustachian tube dysfunction, consequential otitis media, and transient conductive hearing loss occur in 40–45% of head and neck cancer patients during or after radiation therapy [2, 3]. The acute inner ear complications include sensorineural hearing loss (SNHL) and tinnitus [4]. SNHL may occur early after treatment in up to 50% of patients with head and neck tumors treated with radiation therapy [5–7].
5.1 Mechanism
The external ear is a tube covered by skin that conducts sound waves to the middle ear. Radiation effects on the external ear mimics the skin effects of radiation and for mechanism, timing, and symptoms (see Chap. 1).
The mechanism of radiation-induced otitis media is due to swelling of the mucosa following the radiation and subsequent obstruction of the Eustachian tube. The Eustachian tube obstruction results in resorption of the air oxygen and nitrogen from the middle ear, which results in negative pressure and tympanic retraction leading to conductive hearing loss. With further reduction of the negative pressure in the middle ear cavity, fluid transudation takes place resulting in serous otitis media [4, 8].
Stria vascularis in the inner ear is responsible for endolymph production and absorption. Stria vascularis injury after radiation exposure leads to endolymphatic hydrops and temporarily increased intralabyrinthine pressure, which could lead to ear fullness, hearing loss, tinnitus, dizziness, and vertigo [9].
Hearing loss may be conductive, sensorineural, or mixed type. Early hearing loss during radiation therapy is usually conductive due to Eustachian tube dysfunction and radiation-induced otitis media. The incidence of SNHL increases with time, and sensorineural or mixed-type hearing loss occurs either near the end of or shortly after the completion of radiation therapy. The sensory component of early hearing loss is usually related to stria vascularis degeneration and disturbances in normal perilymph and endolymph physiology [9, 10].
5.2 Timing
Acute otitis media usually occurs within a few weeks of radiation therapy. It is usually transient [1] and resolves within a few weeks after completion of the treatment [4].
SNHL may occur near the end of treatment or after the completion of radiation therapy and increase with time. SNHL may be transient or permanent. Transient SNHL could recover within 6–12 months; however, it may last over 12 months in a few cases [5].
Patients with no severe SNHL (less than 30 dB drop from baseline) and no postirradiation serous otitis media have a good chance for recovery of sensorineural hearing within 6 months to 1 year. On the other hand, if severe SNHL develops or the SNHL persists beyond 1 year, it is likely permanent [5].
5.3 Risk Factors
No specific risk factor has been defined for radiation-induced ear toxicities. As with other organs, the maximum dose and ear irradiated volume could affect the prevalence and severity of toxicities. Background skin disease such as lupus erythematous and other autoimmune disease may cause more toxicity for the external ear. Previous middle ear disease such as otitis media or mastoiditis may also increase middle ear radiation-induced toxicities. Concomitant administration of chemotherapy may also increase the risk and severity of otitis in external ear (Fig. 5.1). Platinum-based regimens are used as induction or concurrent chemotherapy in locally advanced head and neck cancers and can potentially affect inner ear toxicity so the risk of SNHL may increase.

Fig. 5.1
External otitis in a patient treated with cisplatin-based chemoradiation of head and neck cancer
5.4 Symptoms and Diagnosis
Symptoms of otitis media are conductive hearing loss, ear pain, fullness, and tinnitus in the affected ear [4]. As a result of radiation therapy, the tympanic membrane may become dull, retracted, bulged, and congested or may remain normal (Fig. 5.2) [3]. An inner ear injury can manifest with tinnitus, dizziness, vertigo, and high-frequency SNHL [5].
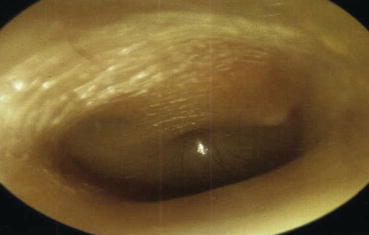
Fig. 5.2
Otitis media after chemoradiation for parotid tumors
Diagnosis of these complications is based on patient symptoms and ear examination including otoscopic assessment. Hearing loss may be diagnosed by simple tests like general assessment of each ear with words spoken at various volumes or a tuning fork or by more thorough audiometry testing. A pure tone audiometer test offers an audiogram based on a person’s ability to hear sounds with different loudness and pitches and characterizes the type and degree of hearing loss.
5.5 Scoring
No distinct grading system has been published for external, middle, and inner ear radiation-induced toxicities separately. Radiation Therapy Oncology Group (RTOG) and the European Organization for Research and Treatment of Cancer (EORTC) have defined the ear toxicity grading system, which considers all three parts as an organ (see Table 5.1) [11].
Table 5.1




RTOG/EORTC ear toxicity scoring
Related posts:



Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
