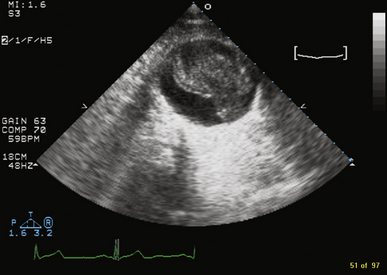
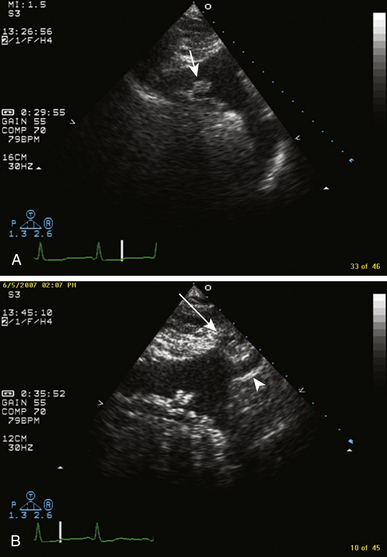
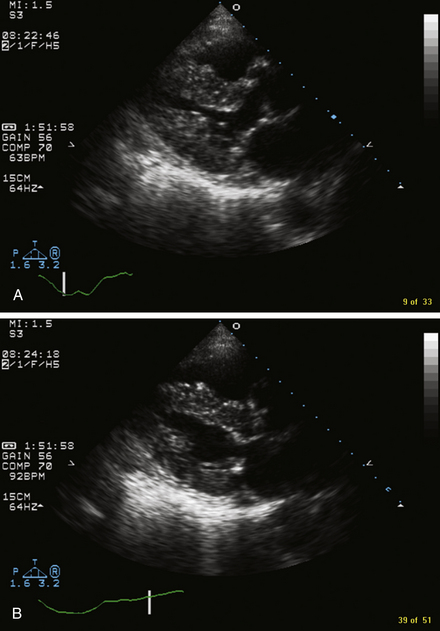
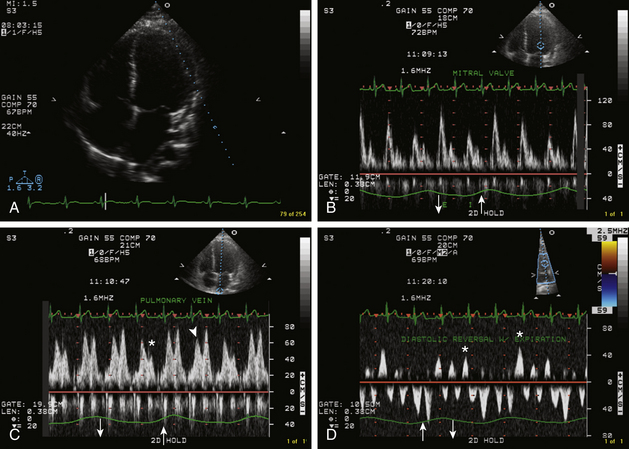
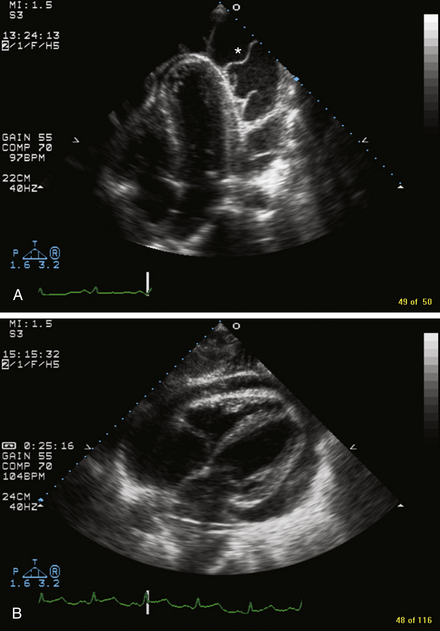
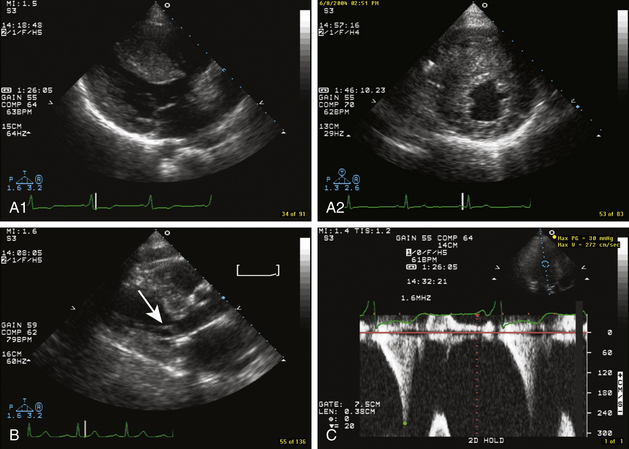
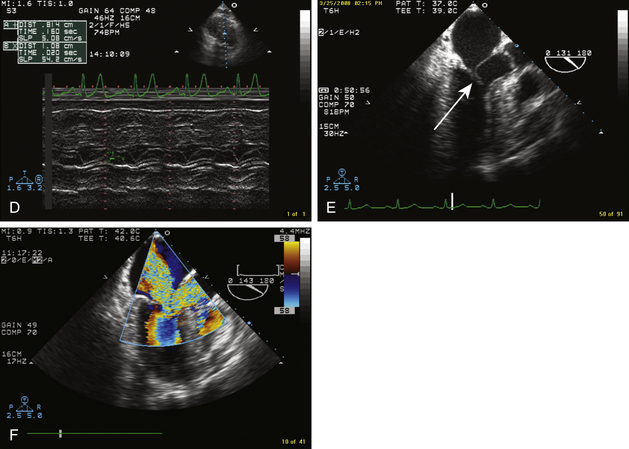
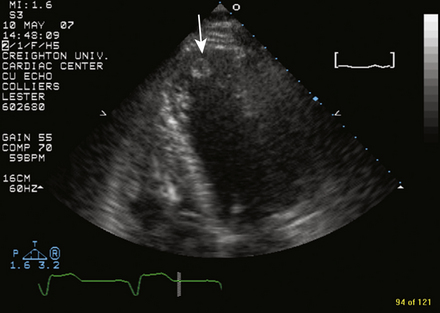
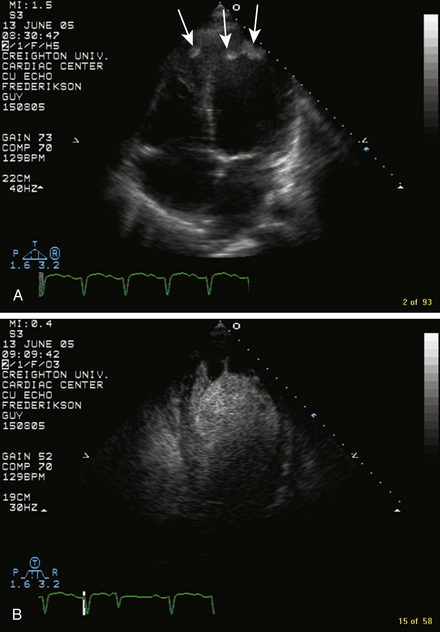
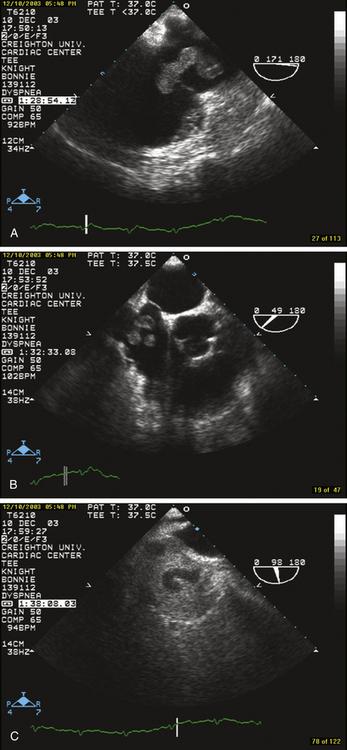
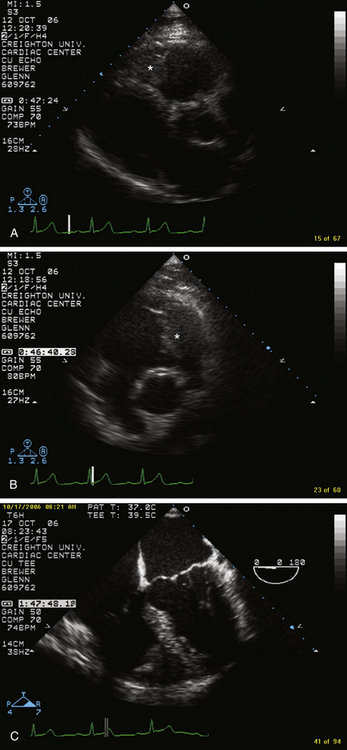
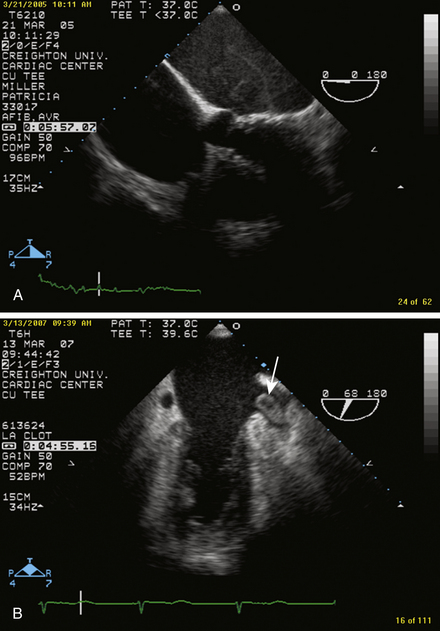
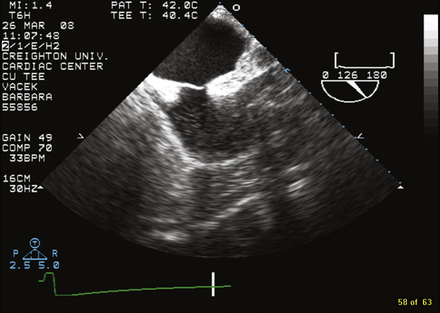
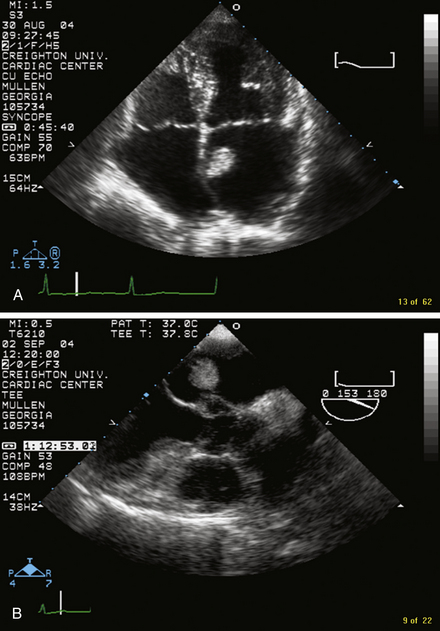
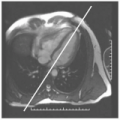
2 Echocardiography FIGURE 2-1 AAA with dissection. Thrombus fills the false lumen. FIGURE 2-2 A, Transthoracic suprasternal notch view of the aortic arch demonstrating severe atheromatous disease of the aortic arch. The pedunculated mass (short arrow) is a mobile atheroma attached to the wall of the aorta by a small stalk. B, Similar view with the origins of the left common carotid (long arrow) and left subclavian (arrowhead) arteries noted. FIGURE 2-3 TEE of an aortic dissection. A, Longitudinal view of the descending thoracic aorta. Note the intimal flap separating the true and false lumens. Color flow imaging shows blood flow within both lumens. B, Transverse view showing the aorta in cross-section with the intimal flap easily visualized. FIGURE 2-4 Parasternal long-axis view in a patient with cardiac amyloidosis. A, Systole. B, Diastole. Important findings are marked concentric LVH with granular speckled appearance of the myocardium. Generally, valve leaflets appear thickened. Although, left ventricular function is often well-preserved until late stages of the disease, diastolic dysfunction is present and is usually restrictive. FIGURE 2-5 TEE of a 29-year-old male with recurrent constrictive pericarditis. The pericardium becomes restrictive and restrains cardiac filling. The volume within the heart nearly becomes fixed. Filling of the cardiac chambers then varies with the respiratory cycle. On inspiration, right ventricular filling increases and left ventricular filling decreases. On expiration, left ventricular filling increases and right ventricular filling decreases. This ventricular interdependence is best demonstrated using pulsed-wave Doppler. A, Apical four-chamber view. The left ventricular size is at the upper limits of normal. B, Pulsed-wave Doppler inflow of the mitral valve with simultaneous use of a respirometer (up arrows indicate inspiration; down arrows indicate expiration). With inspiration, the mitral inflow velocity decreases; with expiration, it increases. The opposite changes in filling velocities occur across the tricuspid valve. C, Pulmonary vein flow demonstrating that both the systolic and diastolic flow velocities decrease at the onset of inspiration (asterisks) and increase at the onset of expiration (arrowhead). D, With expiration, hepatic vein flow diminishes and there is significant diastolic flow reversal (asterisks). FIGURE 2-6 A, Massive pericardial effusion. Transthoracic four-chamber view of an extremely large, circumferential pericardial effusion with fibrinous stranding (asterisk). The right ventricular apex is compressed; note the right atrial collapse in late diastole. B, Subcostal view of another large circumferential pericardial effusion causing tamponade. The size and extent of a pericardial effusion is often best visualized in the subcostal view. FIGURE 2-7 HCM. A, Parasternal long- and short-axis views demonstrating severe concentric LVH. The septum is more severely affected than the other left ventricular walls. B, SAM (short arrow) of the anterior mitral valve leaflet is a hallmark of HCM. It is best seen in the transthoracic parasternal long-axis view. C, Continuous wave Doppler at the level of the LVOT. Note the classic dagger-shaped pattern of flow, which peaks late in systole. The resting gradient measures 30 mm Hg. With Valsalva maneuver, the gradient often increases significantly. D, M-mode through the mitral valve displaying SAM of the anterior mitral valve leaflet. E, Transesophageal three-chamber view clearly showing SAM (long arrow) of the anterior mitral leaflet. This contributes to the dynamic obstruction of blood flow out the LVOT. F, Transesophageal color flow imaging showing increased velocities in the LVOT producing the Venturi effect, essentially pulling the anterior mitral leaflet into the outflow tract. Concurrently, mitral regurgitation occurs. In this example, the mitral regurgitation is severe. FIGURE 2-8 Transthoracic apical four-chamber view in a patient with akinesis of the apex. Note the well-circumscribed echodensity in the left ventricular apex consistent with thrombus (arrow). FIGURE 2-9 A, Apical four-chamber view showing thrombi (arrows) in the left and right ventricular apices in a patient with idiopathic dilated cardiomyopathy. B, With echocontrast the apical thrombi are delineated and appear as dark (shadowed) masses. Echocontrast is commonly used to differentiate thrombus from intracardiac tumor. In an intracardiac tumor, presence of contrast within the mass denotes perfusion of the tumor. FIGURE 2-10 A, Lower esophageal long-axis view of the right heart showing a large wormlike mass traversing the tricuspid valve consistent with thrombus in transit. B, The extensive mobile thrombus is demonstrated again in a midesophageal short-axis view. C, Bicaval transesophageal view during saline contrast injection demonstrating again the mobile thrombus (appears shaded) within the right atrium. This patient was undergoing preoperative evaluation before hip surgery and had been relatively immobile for several weeks. She complained of progressive dyspnea on exertion and right leg swelling for the 2 weeks prior to her examination. She received I.V. TPA and a heparin infusion. On follow-up echocardiography approximately 24 hours later, the thrombus was no longer present. The patient had a complete recovery. FIGURE 2-11 Transthoracic parasternal long- (A) and short-axis (B) views showing a mass (asterisks)within the RV, adherent to the myocardium, extending from the apex to the RVOT. This patient had metastatic renal cell carcinoma. C, The tumor is demonstrated again within the RV in this transverse transesophageal view. This patient received chemotherapy, and the tumor metastases were no longer evident on echocardiography after completion of his treatment. FIGURE 2-12 A, Transverse transesophageal image in a patient with atrial fibrillation. The atria are markedly enlarged and there is significant spontaneous echo contrast visualized within the left atrium. B, Transesophageal longitudinal, two-chamber view revealing a large thrombus (arrow) within the left atrial appendage in another patient with atrial fibrillation. FIGURE 2-13 Longitudinal transesophageal view demonstrating a dumbbell-shaped atrial septum consistent with lipomatous hypertrophy of the septum. Note that fatty infiltration has spared the fossa ovalis. FIGURE 2-14 A, Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related posts: Cardiovascular Computed Tomography Cardiovascular Magnetic Resonance Imaging Angiography Electrocardiography Cardiovascular Magnetic Resonance Imaging Positioning Complete Protocol Example Stay updated, free articles. Join our Telegram channel Join Tags: Cardiovascular Imaging Review Expert Consult Dec 26, 2015 | Posted by admin in CARDIOVASCULAR IMAGING | Comments Off on Echocardiography Full access? Get Clinical Tree
2 Echocardiography FIGURE 2-1 AAA with dissection. Thrombus fills the false lumen. FIGURE 2-2 A, Transthoracic suprasternal notch view of the aortic arch demonstrating severe atheromatous disease of the aortic arch. The pedunculated mass (short arrow) is a mobile atheroma attached to the wall of the aorta by a small stalk. B, Similar view with the origins of the left common carotid (long arrow) and left subclavian (arrowhead) arteries noted. FIGURE 2-3 TEE of an aortic dissection. A, Longitudinal view of the descending thoracic aorta. Note the intimal flap separating the true and false lumens. Color flow imaging shows blood flow within both lumens. B, Transverse view showing the aorta in cross-section with the intimal flap easily visualized. FIGURE 2-4 Parasternal long-axis view in a patient with cardiac amyloidosis. A, Systole. B, Diastole. Important findings are marked concentric LVH with granular speckled appearance of the myocardium. Generally, valve leaflets appear thickened. Although, left ventricular function is often well-preserved until late stages of the disease, diastolic dysfunction is present and is usually restrictive. FIGURE 2-5 TEE of a 29-year-old male with recurrent constrictive pericarditis. The pericardium becomes restrictive and restrains cardiac filling. The volume within the heart nearly becomes fixed. Filling of the cardiac chambers then varies with the respiratory cycle. On inspiration, right ventricular filling increases and left ventricular filling decreases. On expiration, left ventricular filling increases and right ventricular filling decreases. This ventricular interdependence is best demonstrated using pulsed-wave Doppler. A, Apical four-chamber view. The left ventricular size is at the upper limits of normal. B, Pulsed-wave Doppler inflow of the mitral valve with simultaneous use of a respirometer (up arrows indicate inspiration; down arrows indicate expiration). With inspiration, the mitral inflow velocity decreases; with expiration, it increases. The opposite changes in filling velocities occur across the tricuspid valve. C, Pulmonary vein flow demonstrating that both the systolic and diastolic flow velocities decrease at the onset of inspiration (asterisks) and increase at the onset of expiration (arrowhead). D, With expiration, hepatic vein flow diminishes and there is significant diastolic flow reversal (asterisks). FIGURE 2-6 A, Massive pericardial effusion. Transthoracic four-chamber view of an extremely large, circumferential pericardial effusion with fibrinous stranding (asterisk). The right ventricular apex is compressed; note the right atrial collapse in late diastole. B, Subcostal view of another large circumferential pericardial effusion causing tamponade. The size and extent of a pericardial effusion is often best visualized in the subcostal view. FIGURE 2-7 HCM. A, Parasternal long- and short-axis views demonstrating severe concentric LVH. The septum is more severely affected than the other left ventricular walls. B, SAM (short arrow) of the anterior mitral valve leaflet is a hallmark of HCM. It is best seen in the transthoracic parasternal long-axis view. C, Continuous wave Doppler at the level of the LVOT. Note the classic dagger-shaped pattern of flow, which peaks late in systole. The resting gradient measures 30 mm Hg. With Valsalva maneuver, the gradient often increases significantly. D, M-mode through the mitral valve displaying SAM of the anterior mitral valve leaflet. E, Transesophageal three-chamber view clearly showing SAM (long arrow) of the anterior mitral leaflet. This contributes to the dynamic obstruction of blood flow out the LVOT. F, Transesophageal color flow imaging showing increased velocities in the LVOT producing the Venturi effect, essentially pulling the anterior mitral leaflet into the outflow tract. Concurrently, mitral regurgitation occurs. In this example, the mitral regurgitation is severe. FIGURE 2-8 Transthoracic apical four-chamber view in a patient with akinesis of the apex. Note the well-circumscribed echodensity in the left ventricular apex consistent with thrombus (arrow). FIGURE 2-9 A, Apical four-chamber view showing thrombi (arrows) in the left and right ventricular apices in a patient with idiopathic dilated cardiomyopathy. B, With echocontrast the apical thrombi are delineated and appear as dark (shadowed) masses. Echocontrast is commonly used to differentiate thrombus from intracardiac tumor. In an intracardiac tumor, presence of contrast within the mass denotes perfusion of the tumor. FIGURE 2-10 A, Lower esophageal long-axis view of the right heart showing a large wormlike mass traversing the tricuspid valve consistent with thrombus in transit. B, The extensive mobile thrombus is demonstrated again in a midesophageal short-axis view. C, Bicaval transesophageal view during saline contrast injection demonstrating again the mobile thrombus (appears shaded) within the right atrium. This patient was undergoing preoperative evaluation before hip surgery and had been relatively immobile for several weeks. She complained of progressive dyspnea on exertion and right leg swelling for the 2 weeks prior to her examination. She received I.V. TPA and a heparin infusion. On follow-up echocardiography approximately 24 hours later, the thrombus was no longer present. The patient had a complete recovery. FIGURE 2-11 Transthoracic parasternal long- (A) and short-axis (B) views showing a mass (asterisks)within the RV, adherent to the myocardium, extending from the apex to the RVOT. This patient had metastatic renal cell carcinoma. C, The tumor is demonstrated again within the RV in this transverse transesophageal view. This patient received chemotherapy, and the tumor metastases were no longer evident on echocardiography after completion of his treatment. FIGURE 2-12 A, Transverse transesophageal image in a patient with atrial fibrillation. The atria are markedly enlarged and there is significant spontaneous echo contrast visualized within the left atrium. B, Transesophageal longitudinal, two-chamber view revealing a large thrombus (arrow) within the left atrial appendage in another patient with atrial fibrillation. FIGURE 2-13 Longitudinal transesophageal view demonstrating a dumbbell-shaped atrial septum consistent with lipomatous hypertrophy of the septum. Note that fatty infiltration has spared the fossa ovalis. FIGURE 2-14 A, Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related posts: Cardiovascular Computed Tomography Cardiovascular Magnetic Resonance Imaging Angiography Electrocardiography Cardiovascular Magnetic Resonance Imaging Positioning Complete Protocol Example Stay updated, free articles. Join our Telegram channel Join Tags: Cardiovascular Imaging Review Expert Consult Dec 26, 2015 | Posted by admin in CARDIOVASCULAR IMAGING | Comments Off on Echocardiography Full access? Get Clinical Tree