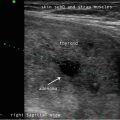
Fig. 8.1
(a, b) SWE values of 9.6 and 12.6 kPa in a normal thyroid using 3 N and 5 N of force, respectively
8.5.2 Thyroid Inflammation
Inflammation and fibrosis are very common in the thyroid gland and often coexist with thyroid nodules. The influence of concomitant thyroiditis on the elasticity of thyroid nodules is still a matter of debate. According to some authors, Hashimoto’s thyroiditis, or chronic autoimmune thyroiditis, does not significantly affect the coexisting nodules’ stiffness [39–41]. However, acute or subacute thyroiditis may cause more significant changes in elasticity of the thyroid parenchyma in general and therefore may influence the elasticity measurement of coexistent thyroid nodules [42]. Therefore, postponing the evaluation of the nodule stiffness until complete recovery from acute or subacute thyroiditis is recommended [43]. Figure 8.2 represents a shear wave elastogram of a patient who was diagnosed with a benign follicular adenoma (oncocytic type) in the setting of chronic lymphocytic (Hashimoto’s) thyroiditis. As seen in the image, the SWE value of 28.55 kPa would qualify this subject as a malignant nodule based on the cutoff value of 22.3 kPa proposed by Samir et al. [14].

Fig. 8.2
A 50-year-old female with a right thyroid nodule that was suspicious for a Hurthle cell neoplasm on FNA. The elastogram shows a SWE value of 28.55 kPa. The patient underwent a total thyroidectomy, and the nodule was a benign follicular adenoma (oncocytic type) in the setting of chronic lymphocytic (Hashimoto’s) thyroiditis
8.5.3 Cyst Fluid and Calcifications
The fluid within a thyroid nodule may affect the elasticity measurements. Interestingly, the stiffness of benign nodules with a cystic component was higher than solid ones [40, 44]. This finding may be related to the pressure exerted by the liquid contained in the cystic compartment [44]. The presence of both micro- and macrocalcifications may influence the stiffness of thyroid nodules. In particular, macrocalcifications around or within a nodule may lead to a significant increase in elasticity (Fig. 8.3). In nodules with both types of calcifications, the influence might be more pronounced [40]. Due to the possibility of a false-positive result, thyroid nodules with coarse calcifications may not be suitable for elastographic examination [45].

Fig. 8.3
A 85-year-old female with a left thyroid nodule measuring 2.6 cm, FLUS on FNA. The final pathology after surgery was a benign Hurthle cell adenoma with extensive calcification. As seen in the elastogram, the calcification causes significant elasticity increase
It may be possible to perform the quantitative measurements by placing the ROI on the target nodule with the calcified or cystic areas avoided; however, this may not be feasible when the solid area is less than the sampling size of ROI.
8.6 Conclusions
In conclusion, elastography is a relatively noninvasive test that could increase the specificity of conventional ultrasound in the differentiation between malignant and benign thyroid nodules. Furthermore, the combination of this technique and conventional ultrasound may be a valuable tool in the identification of nodules that require FNAB and in nodules with indeterminate or nondiagnostic cytology . However, the general limitations described above should be acknowledged. It may be that the best and most appropriate application of elastography in the diagnosis of thyroid nodules will be as a complement to conventional ultrasound and FNAB with genetic testing [46].
References
1.
2.
Tumbridge WM, Evered DC, Hall R, et al. The spectrum of thyroid disease in a community: the Whick-ham survey. Clin Endocrinol (Oxf). 1997;7:481–93.CrossRef
3.
4.
Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26(1):1–133.CrossRefPubMedPubMedCentral
5.
Dhyani M, Faquin W, Lubitz CC, Daniels GH, Samir AE. How to interpret thyroid fine-needle aspiration biopsy reports: a guide for the busy radiologist in the era of the Bethesda classification system. Am J Roentgenol. 2013;201(6):1335–9.CrossRef
6.
7.
8.
9.
10.
Friedrich-Rust M, Meyer G, Dauth N, et al. Interobserver agreement of Thyroid Imaging Reporting and Data System (TIRADS) and strain elastography for the assessment of thyroid nodules. PLoS One. 2013;8(10):e77927.CrossRefPubMedPubMedCentral
Related posts:
 Ultrasound-Guided Laser Ablation
Ultrasound-Guided Laser Ablation
 Ultrasound as a Component of Medical School Curriculum/Simulation Training
Ultrasound as a Component of Medical School Curriculum/Simulation Training
 Intraoperative Use of Ultrasound in Thyroid, Parathyroid, and Cervical Lymph Node Surgery
Intraoperative Use of Ultrasound in Thyroid, Parathyroid, and Cervical Lymph Node Surgery
 Parathyroid Ultrasound Imaging: Pearls, Pitfalls, and Tips
Parathyroid Ultrasound Imaging: Pearls, Pitfalls, and Tips
 Feature Illustration: Vascularity
Feature Illustration: Vascularity
 Pattern Recognition: Diffuse Thyroid Disease
Pattern Recognition: Diffuse Thyroid Disease
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


