theoretical treatment of this subject is given elsewhere (2, 3, 4, 5), it will suffice here to provide some important generalizations.
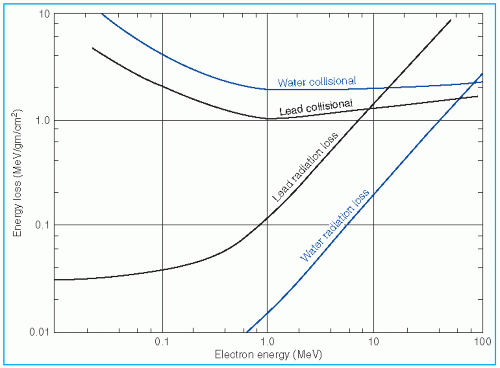 Figure 14.1. Rate of energy loss in MeV per g/cm2 as a function of electron energy for water and lead. (From Johns HE, Cunningham JR. The Physics of Radiology. 3rd ed. Springfield, IL: Charles C Thomas; 1969, with permission.) |

 , the absorbed dose, D, is closely approximated by
, the absorbed dose, D, is closely approximated by
 , where
, where  is the mean square scattering angle. Following the calculations of Rossi (13), mass scattering powers for various materials and electron energies have been tabulated (14).
is the mean square scattering angle. Following the calculations of Rossi (13), mass scattering powers for various materials and electron energies have been tabulated (14).threshold energy for nuclear reactions; range measurements; and the measurement of Cerenkov radiation threshold (14). Of these, the range method is the most practical and convenient for clinical use.
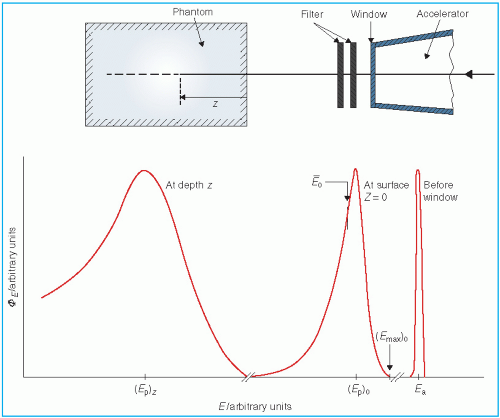 Figure 14.2. Distribution of electron fluence in energy, øE, as the beam passes through the collimation system of the accelerator and the phantom. (From International Commission on Radiation Units and Measurements. Radiation Dosimetry: Electrons with Initial Energies between 1 and 50 MeV. Report No. 21. Washington, DC: International Commission on Radiation Units and Measurements; 1972, with permission.) |
 , where f is the effective source to surface distance (SSD); see Section 14.4E for details) and z is the depth. However, this correction in Rp is clinically not significant in terms of its impact on the ionization to dose conversion factor (20).
, where f is the effective source to surface distance (SSD); see Section 14.4E for details) and z is the depth. However, this correction in Rp is clinically not significant in terms of its impact on the ionization to dose conversion factor (20).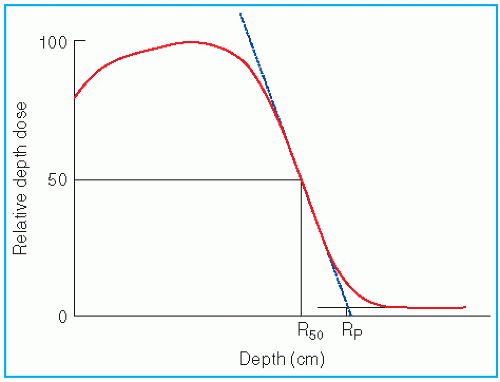 Figure 14.3. Depth dose curve illustrating the definition of Rp and R50. |


 , as a function of mean electron energy at depth; and (b) chamber replacement correction, Prepl. This factor is dependent both on the air cavity diameter as well as well as the mean electron energy at the depth of measurement.
, as a function of mean electron energy at depth; and (b) chamber replacement correction, Prepl. This factor is dependent both on the air cavity diameter as well as well as the mean electron energy at the depth of measurement. are provided in the Appendix (Table A.3) as a function of incident electron beam energy and depth. The factor Prepl accounts for three effects: (a) the in-scatter effect, which increases the electron fluence in the chamber cavity because of electron scattering out of the air cavity being less than that expected in the intact medium; (b) the obliquity effect, which decreases the fluence in the cavity because of electrons travelling relatively straight in the air cavity instead of taking oblique paths as they would without cavity owing to larger-angle scattering in the medium than air; and (c) the displacement in the effective point of measurement. The first two effects may be grouped into a fluence correction, while the third is called the gradient correction.
are provided in the Appendix (Table A.3) as a function of incident electron beam energy and depth. The factor Prepl accounts for three effects: (a) the in-scatter effect, which increases the electron fluence in the chamber cavity because of electron scattering out of the air cavity being less than that expected in the intact medium; (b) the obliquity effect, which decreases the fluence in the cavity because of electrons travelling relatively straight in the air cavity instead of taking oblique paths as they would without cavity owing to larger-angle scattering in the medium than air; and (c) the displacement in the effective point of measurement. The first two effects may be grouped into a fluence correction, while the third is called the gradient correction.
TABLE 14.1 Effective Density for Scaling Depth in Nonwater Phantoms to Water for Electron Beamsa | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||
 correction as a function of depth still needs to be applied.
correction as a function of depth still needs to be applied.relative dosimetry. Care is required to avoid air gaps adjacent to the film. In addition, the sensitometric curve (optical density as a function of absorbed dose) must be known to interpret the optical density in terms of absorbed dose. Wherever possible, a film with a linear response over the range of measured dose should be used. Errors caused by changes in the processing conditions can be minimized by developing the films at approximately the same time. Accuracy can also be improved by using films from the same batch.
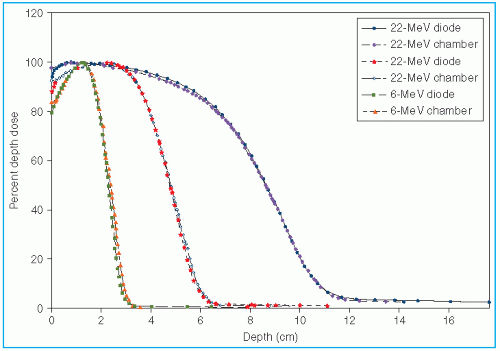 Figure 14.4. Comparison of depth dose curves measured with a diode and an ion chamber. Whereas the diode response was uncorrected, the chamber readings were corrected for change in  as a function of depth, and the displacement of the effective point of measurement. (From Khan FM. Clinical electron beam dosimetry. In: Keriakes JG, Elson HR, Born CG, eds. Radiation Oncology Physics—1986. AAPM Monograph No. 15. New York, NY: American Institute of Physics; 1986:211, with permission.) as a function of depth, and the displacement of the effective point of measurement. (From Khan FM. Clinical electron beam dosimetry. In: Keriakes JG, Elson HR, Born CG, eds. Radiation Oncology Physics—1986. AAPM Monograph No. 15. New York, NY: American Institute of Physics; 1986:211, with permission.) |
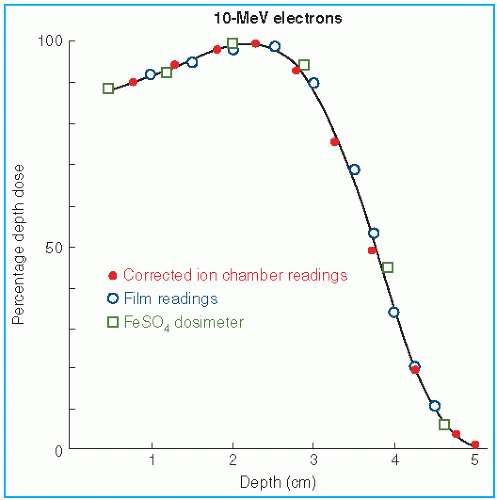 Figure 14.5. Comparison of central axis depth dose curve measured with an ion chamber, film, and FeSO4 dosimeter. (From Almond PR. Calibration of megavoltage electron radiotherapy beams. In: Waggener RG, Kereiakes JG, Shalek RJ, eds. Handbook of Medical Physics, Vol 1. Boca Raton, FL: CRC Press; 1982:173, with permission.) |

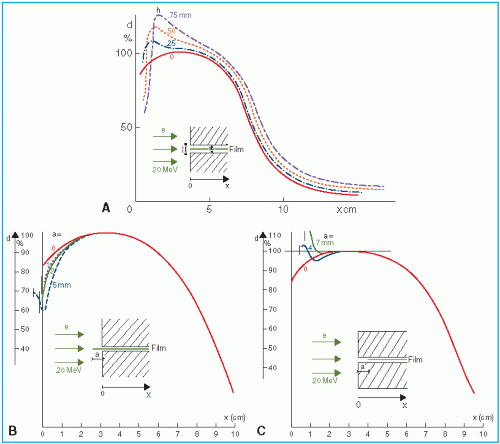 Figure 14.6. Film artifacts created by misalignment of the film in the phantom. The effects of A: air gaps between the film and the phantom, B: film edge extending beyond the phantom, and C: film edge recessed within the phantom. (From Dutreix J, Dutreix A. Film dosimetry of high energy electrons. Ann NY Acad Sci. 1969;161:33, with permission.) |
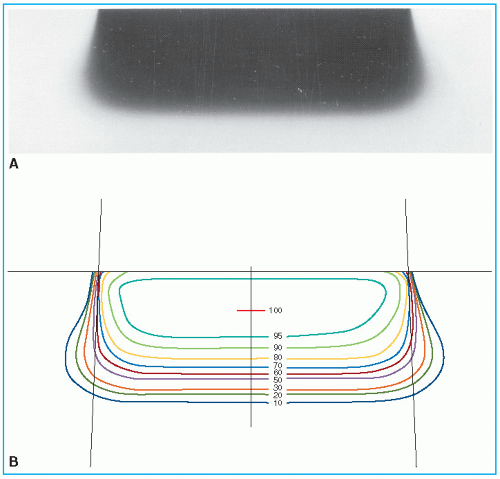 Figure 14.7. Film used for obtaining isodose curves. A: A film exposed to 12-MeV electron beam, 14 × 8-cm cone, in a polystyrene phantom. B: Isodensity curves. |
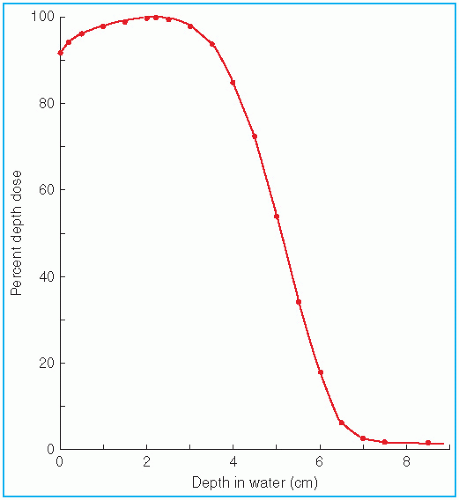 Figure 14.8. Central axis depth dose distribution measured in water. Incident energy (Ep)0 = 13 MeV; 8 × 10-cm cone; effective source to surface distance = 68 cm. |
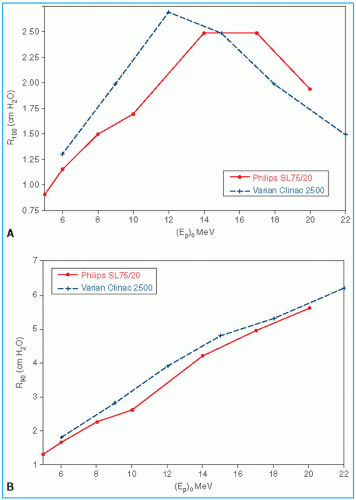 Figure 14.9. Plots of depth dose ranges as a function of the most probable energy (Ep)0 at the surface for two different linear accelerators. A: R100, the depth of maximum dose versus (Ep)0. B: R90, the depth of 90% depth dose versus (Ep)0. (From Khan FM. Clinical electron beam dosimetry. In: Keriakes JG, Elson HR, Born CG, eds. Radiation Oncology Physics—1986. AAPM Monograph No. 15. New York, NY: American Institute of Physics; 1986:211, with permission.) |
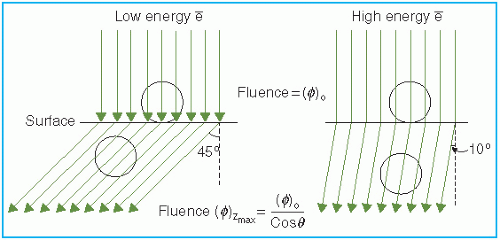 Figure 14.10. Schematic illustration showing the increase in percent surface dose with an increase in electron energy. (From Khan FM. Clinical electron beam dosimetry. In: Keriakes JG, Elson HR, Born CG, eds. Radiation Oncology Physics—1986. AAPM Monograph No. 15. New York, NY: American Institute of Physics; 1986:211, with permission.) |
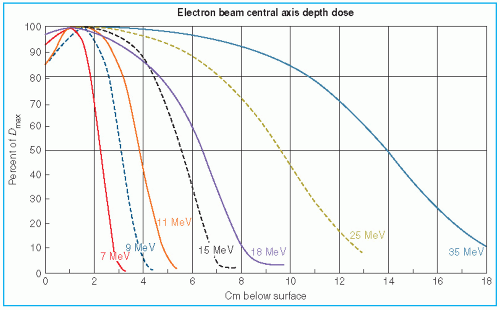 Figure 14.11. Comparison of central axis depth dose distributions of the Sagittaire linear accelerator (continuous curves) and the Siemen’s betatron (dashed curves). (From Tapley N, ed. Clinical Applications of the Electron Beam. New York, NY: John Wiley & Sons; 1976, with permission.) |
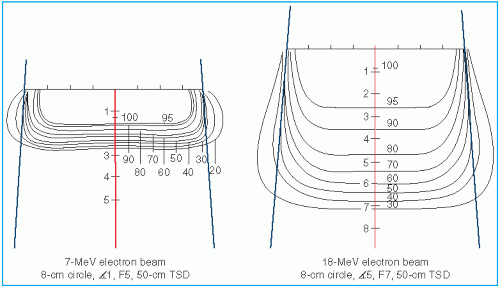 Figure 14.12. Comparison of isodose curves for different energy electron beams. (From Tapley N, ed. Clinical Applications of the Electron Beam. New York, NY: John Wiley & Sons; 1976:86, with permission.) |
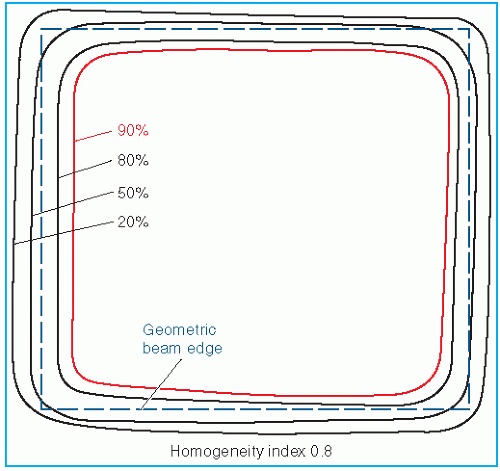 Figure 14.13. Isodose curves in a plane perpendicular to the central axis, obtained with a film placed in a phantom at the depth of maximum dose. (From Almond PR. Radiation physics of electron beams. In: Tapley N, ed. Clinical Applications of the Electron Beam. New York, NY: John Wiley & Sons; 1976:50, with permission.) |
a desired degree of beam widening and flattening. Analysis by Werner et al. (34) shows that the dual-foil systems compare well with the scanning beam systems in minimizing angular spread and, hence, the effect on dose distribution characteristics.
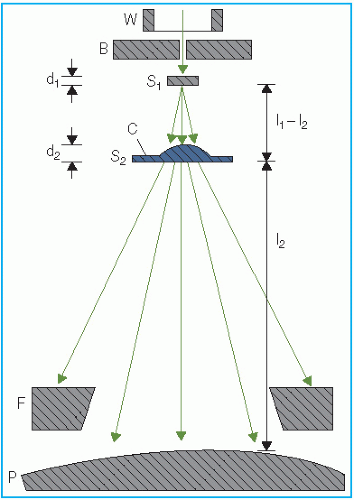 Figure 14.14. Principle of dual-foil system for obtaining uniform electron beam field. (From Almond PR. Handbook of Medical Physics. Vol I. Boca Raton, FL: CRC Press; 1982:149, with permission.) |
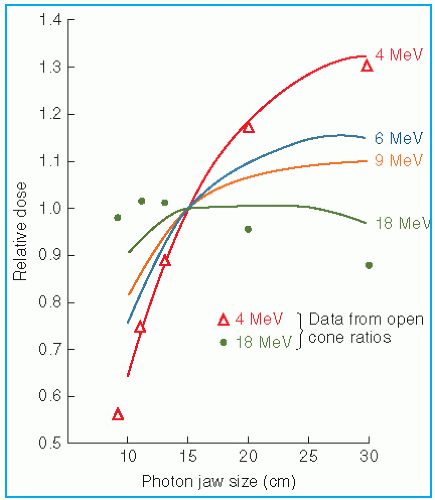 Figure 14.15. Variation of relative dose at dmax, through a 10 × 10-cm cone, with change of jaw setting, relative to the recommended jaw setting. (From Biggs PJ, Boyer AL, Doppke KP. Electron dosimetry of irregular fields on the Clinac-18. Int J Radiat Oncol Biol Phys. 1979;5:433, with permission.) |
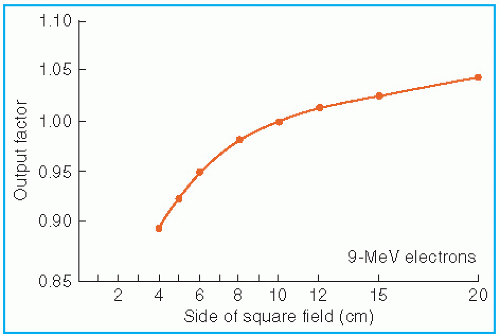 Figure 14.16. Output factors as a function of side of the square field. Primary collimator fixed, secondary collimators (trimmers) close to the phantom varied to change the field size. Data are from Therac 20 linear accelerator. (From Mills MD, Hogstrom KR, Almond PR. Prediction of electron beam output factors. Med Phys. 1982;9:60, with permission.) |
incident fluence and cross-sectional beam uniformity, the equivalent fields have the same depth dose distribution along the central ray. Thus, field equivalence here is defined in terms of PDDs and not the output factors, which depend on particular jaw setting for the given applicator or other collimation conditions. According to this definition, all broad fields are equivalent because their depth dose distribution is the same irrespective of field size. For example, 10 × 10, 10 × 15, 10 × 20, and 20 × 20 are all broad fields for energies up to 30 MeV (see Equation 14.11) and hence are equivalent in depth dose distribution. Field equivalence is therefore relevant only for small fields in which the LSE does not exist, and consequently, the depth dose distribution is field size dependent.
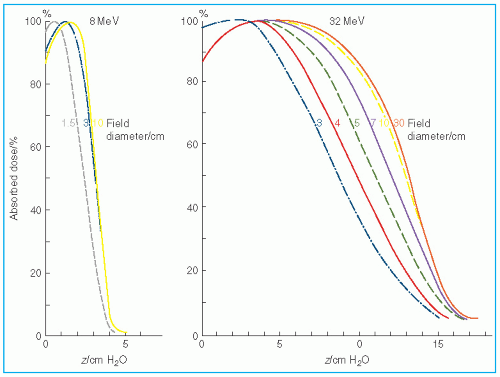 Figure 14.17. Variation of depth dose distribution with field size. (From International Commission on Radiation Units and Measurements. Radiation Dosimetry: Electron Beams with Energies between 1 and 50 MeV. Report No. 35. Bethesda, MD: International Commission on Radiation Units and Measurements; 1984, with permission.) |
effective SSD is defined as the distance from an effective source position to the standard phantom position (e.g., isocenter) which gives the correct inverse square law relationship for the change in output with distance. Khan et al. (44) have recommended a method that simulates as closely as possible the clinical situation. In this method, doses are measured in a phantom at the depth of maximum dose (dm), with the phantom first at the standard SSD (zero gap) and then at various distances, up to about 20 cm from the applicator end. Suppose f = effective SSD, I0 = dose with zero gap, and Ig = dose with gap g between the standard SSD point and the phantom surface. Then, if electrons obey inverse square law,


 as a function of gap g (Fig. 14.19), a straight line is obtained, the slope of which is
as a function of gap g (Fig. 14.19), a straight line is obtained, the slope of which is  . Thus the effective SSD is given by
. Thus the effective SSD is given by  .
.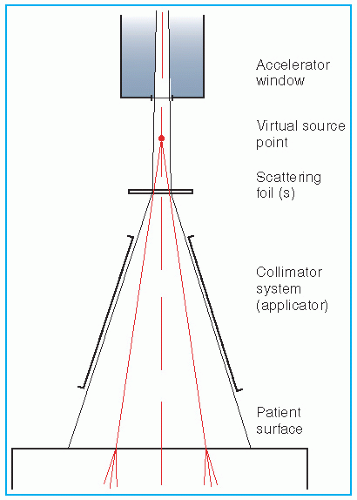 Figure 14.18. Definition of the virtual point source of an electron beam: the intersection point of the backprojections along the most probable directions of motion of electrons at the patient surface. (From Schroeder-Babo P. Determination of the virtual electron source of a betatron. Acta Radiol. 1983;364(suppl):7, with permission.) |
scattering foils are not used. In a modern linear accelerator, typical x-ray contamination dose to a patient ranges from approximately 0.5% to 1% in the energy range of 6 to 12 MeV; 1% to 2%, from 12 to 15 MeV; and 2% to 5%, from 15 to 20 MeV.
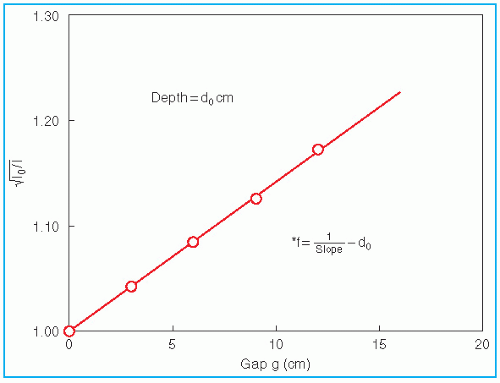 Figure 14.19. Determination of the effective source to surface distance. (From Khan FM, Sewchand W, Levitt SH. Effect of air space on depth dose in electron beam therapy. Radiology. 1978;126:249, with permission.) |
TABLE 14.2 X-ray Contamination Dose (Dx) to Water, at the End of the Electron Range as a Percentage of Dmax | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


