Chapter 3 Electronic fetal monitoring: terminology
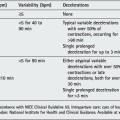
Even when we all speak one language there remain difficulties in communication because of differing use of terminology. This may be resolved by better understanding and consideration of terms and definitions agreed by the International Federation of Obstetrics and Gynaecology (FIGO) Subcommittee on Standards in Perinatal Medicine. These recommendations were published in 1987 in the International Journal of Gynecology and Obstetrics.12 Recently the National Institute for Clinical Excellence (NICE) has published guidelines on fetal monitoring and they are largely used in this text.13 Without a consistency of terminology we cannot have a consistency of interpretation.
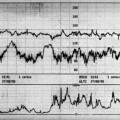
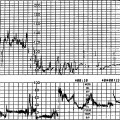
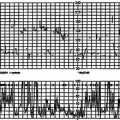
A fetal heart rate tracing should be technically adequate to warrant analysis. The pen heat should not be too high because it can produce a very dark trace, occasionally burning the paper, or too low, producing a faint trace. This can be adjusted on most machines; however, it is also affected by using the incorrect paper for the machine. The length of the CTG strip depends on the paper speed. In the UK it is usually 1 cm/min while in the USA it is 3 cm/min. As the pattern of the trace is dramatically altered by a change in paper speed this can lead to confusion. It should, therefore, be standardized. Because there is not much to be gained by the faster paper speed with a consequent greater consumption of paper the slower speed of 1 cm/min should be selected. Each vertical division on the paper is 1 cm and therefore 1 min. A tracing should be annotated fully. At the beginning of the trace the mother’s name, reference number and pulse rate should be recorded. Modern machines automatically annotate the time and date; however, a human being has to ensure that they are correctly set in the software and changed as the clock time changes, notably with the onset of ‘summer time’. The newest monitors have keypads or bar-code readers with which any other information may be recorded on the trace. It is important to relate vaginal examination, change of posture, epidural and other transient events to the fetal heart rate pattern, which could have medico-legal implications at a later date. The vertical scale on the paper should be standardized to display between 50 and 210 beats per min (bpm) in order for visual perception and interpretation to be consistent.
A tracing should be annotated fully.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


