CHAPTER 1
Embryology and Physiology of the Fetal Heart
Congenital heart disease is the most common severe congenital abnormality found among live births.1–13
Because development of the heart is an interaction of genes, environment, and chance, approximately 70% to 85% of cases of congenital heart disease have multifactorial causes.14–17
Embryology
All major organ systems are formed between the fourth and eighth weeks of development (Table 1–1). This is called the period of organogenesis. It is during this time that the embryo is most susceptible to factors that interfere with development.
TABLE 1–1
Timing of Embryologic Heart Formation
| Timing | Event |
| Days 21–22 | Umbilical veins, vitelline veins, cardinal veins form |
| Single heart tube forms | |
| Pericardial cavity forms | |
| Day 23 | Heart tube grows rapidly, forcing it to fold on itself |
| Days 25–28 | Atrioventriculobulbar loop forms |
| Common atrium forms | |
| Atrioventricular canal forms connecting common atrium to early embryonic ventricles | |
| Septum primum appears | |
| Days 27–37 | Endocardial cushions appear |
| Day 28 | Heart begins to beat |
| Ventricular septum appears as a small ridge in common ventricle | |
| Ventricles begin to dilate | |
| Days 28–35 | Absorption of bulbous cordis and sinus venosus |
| Four-chambered heart forms | |
| Day 29 | Pulmonary veins form |
| Days 31–35 | Placental circulation begins |
| Atrioventricular node develops | |
| Ostium secundum is formed | |
| Sinoatrial node develops | |
| Day 33 | Tricuspid and mitral valves form |
| Days 35–42 | Coronary arteries form |
| Days 36–42 | Inferior vena cava forms |
| Days 43–49 | Superior vena cava forms |
| Coronary sinus forms | |
| Day 49 | Formation of muscular interventricular septum |
| Day 56 | Aorta and pulmonary arteries form |
| Aortic and pulmonic valves form |
The cardiovascular system, including the heart, blood vessels, and blood cells, originates from the mesodermal germ layer.18 Cardiovascular morphogenesis is controlled by mechanisms that are common to all developmental processes: cell growth, cell migration, cell death, differentiation, and adhesion.
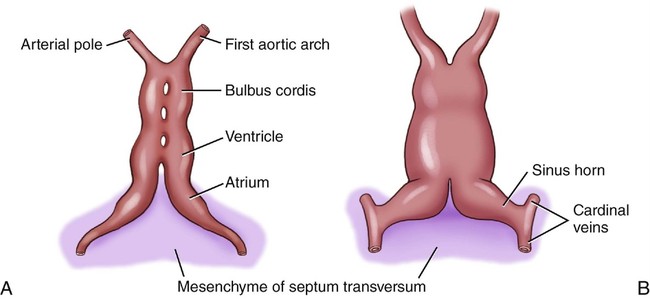
The heart initially consists of paired tubular structures that by the twenty-second day of development (the embryo is approximately 2.5 to 3 mm in length) form a single, slightly bent heart tube (Fig. 1–1). This heart tube consists of an inner endocardial tube and a surrounding myoepicardial mantle. At this stage, the heart tube connects with the developing arch system and with the vitelline and umbilical veins.19
The second stage of cardiac development begins with the formation of the atrioventriculobulbar loop. The cephalic portion of the heart tube bends ventrally and to the right, whereas the caudal atrial portion begins to bend in a dorsocranial direction and to the left, thus forming a loop (Fig. 1–2).18
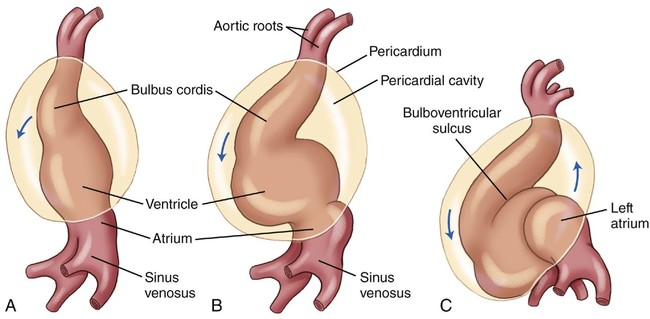
It is at this time (approximately 28 days) that contractions are thought to begin in the ventriculobulbar portion of the heart, and the heart beat is initiated.20 Circulation occurs from the sinus venosus into the right atrium, into the left atrium, and then into the atrioventricular canal and the ventricles.
Stage three in the development of the heart consists of absorption of the bulbus cordis and sinus venosus. At this stage, the atrioventriculobulbar loop begins to untwist and the cardiac septa develop, forming a four-chambered heart.19
Formation of the septa within the heart results from the development of endocardial cushion tissue in the atrioventricular canal and the truncoconal region. This occurs between the twenty-seventh and thirty-seventh days of development, when the embryo is 4 to 14 mm in length (Fig. 1–3).
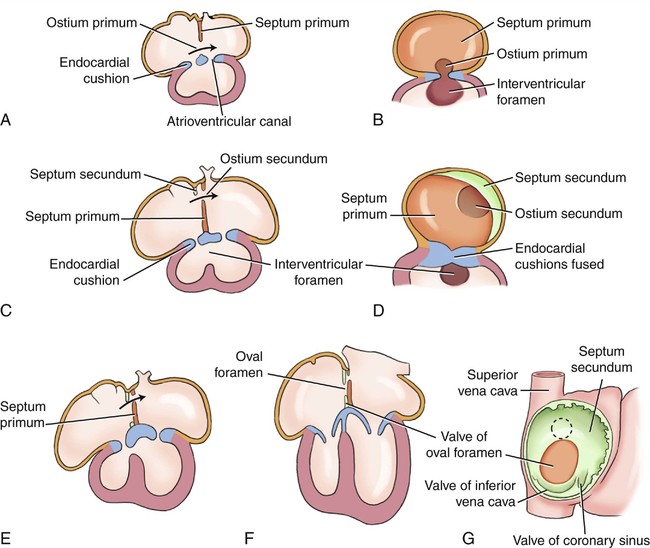
Last, a septum secundum is formed, but an interatrial opening, the foramen ovale, remains until birth when pressure in the left atrium increases, causing the two septa to press against each other and close this communication.20
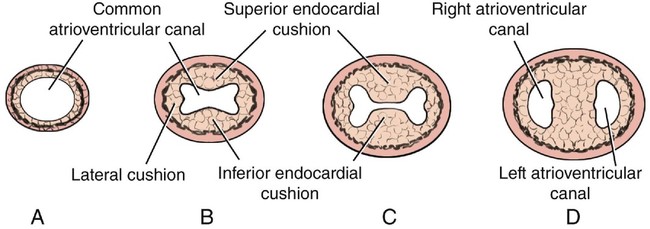
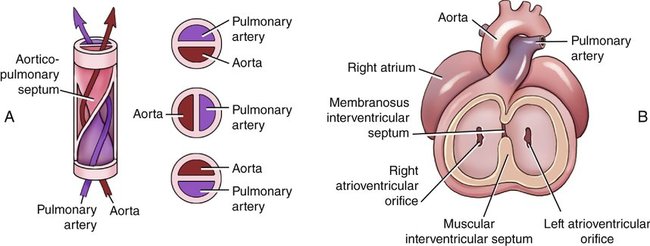
Septum formation within the atrioventricular canal occurs when two large endocardial cushions fuse, resulting in a right (tricuspid) and left (mitral) atrioventricular orifice (Fig. 1–4). This usually occurs by day 33 of development.18
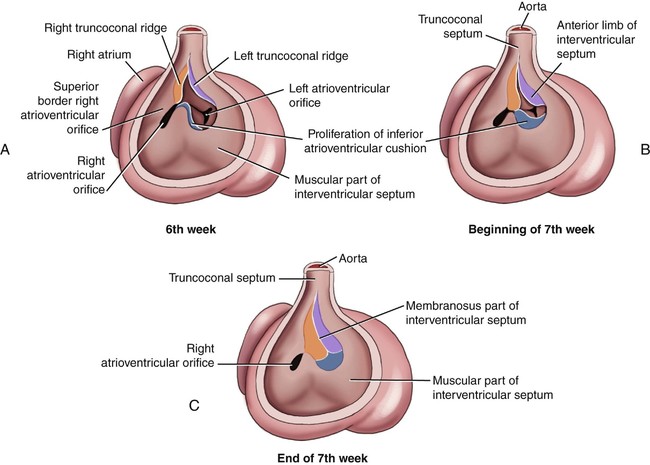
The interventricular septum is formed by the end of the seventh week of development (Fig. 1–5). It results from the dilation of the two primitive ventricles (right and left conus swellings), which causes the medial walls to become apposed and fuse together. This forms the muscular portion of the interventricular septum. Formation of the membranous portion follows.
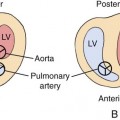
During the eighth week of development, the truncus swellings or cushions of the primitive heart grow and twist around each other to form the aorticopulmonary septum (Fig. 1–6). This septum divides the truncus arteriosus into an aortic channel and a pulmonary channel.
Next, the opening that remained between the two ventricles closes as a result of the conus septum fusing with tissue from the inferior endocardial cushions along the top of the muscular interventricular septum (see Fig. 1–5). This becomes the membranous part of the interventricular septum.18,19
Between 5 and 7 weeks of development, the semilunar valves (aortic and pulmonic valves) are formed.
Aortic Arches
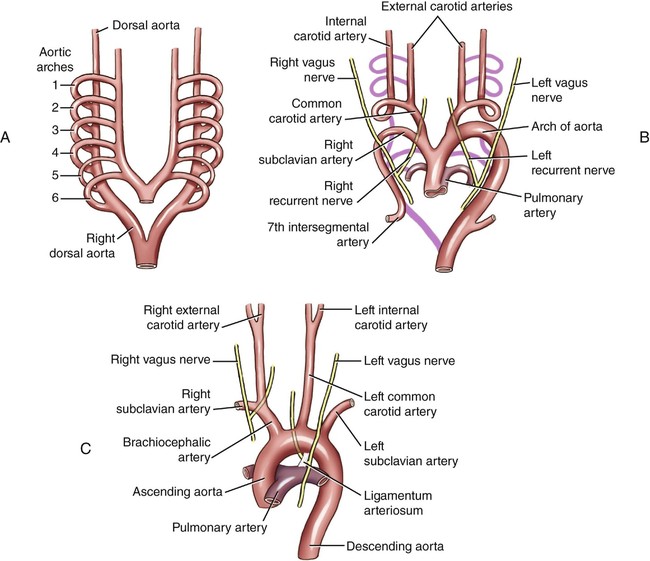
During the fourth and fifth weeks of development, six pairs of arteries arising from the most distal portion of the truncus arteriosus are formed (Table 1–2). They are known as aortic arches (Fig. 1–7). These arches form communications between the aortic sac and the two dorsal aortas.
TABLE 1–2
Timing of Aortic Arch Formation
| Timing | Event |
| Days 19–20 | First pair of aortic arches form |
| Days 20–23 | Second pair of aortic arches form |
| Days 24–25 | Third pair of aortic arches form |
| First and second pairs of aortic arches disappear | |
| Third pair of aortic arches becomes the internal carotid arteries | |
| Days 26–30 | Fourth pair of aortic arches form |
| Fourth left arch becomes the definitive aorta | |
| Fourth right arch becomes the right subclavian artery | |
| Fifth pair of aortic arches never fully develop | |
| Day 30 | Sixth pair of aortic arches form |
| Sixth right arch becomes right pulmonary artery | |
| Sixth left arch becomes left pulmonary artery (ductus arteriosus) |



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


