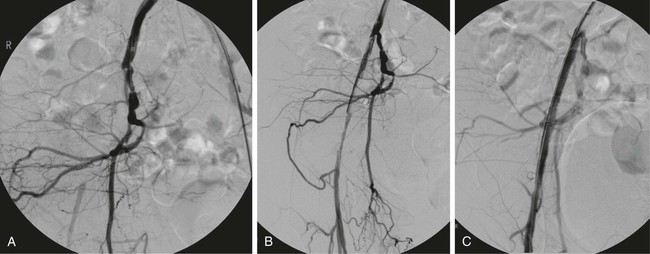
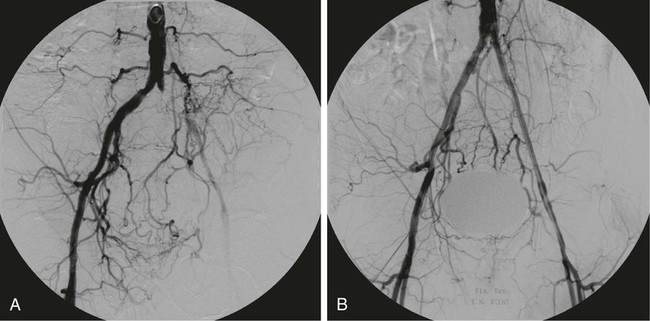
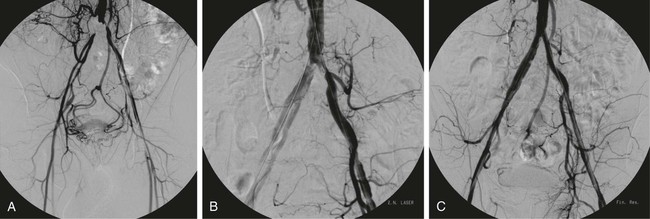
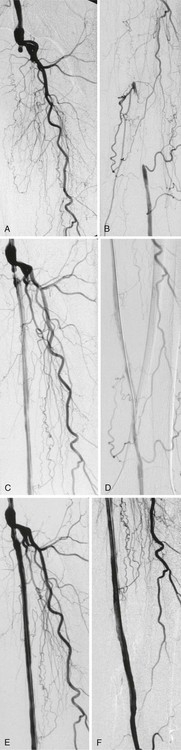
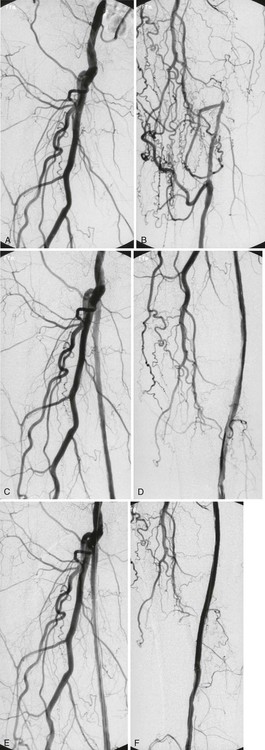
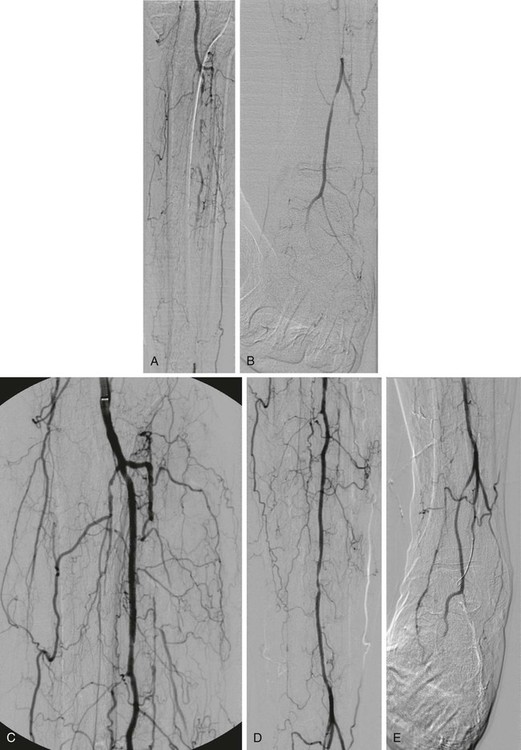
Chapter 13 Jörn O. Balzer and Verena Kahn Chronic atherosclerotic obstructions are a leading cause of lifestyle-limiting intermittent claudication that occurs in 3% to 20% of the population older than 60 years of age.1 With the introduction of percutaneous revascularization techniques, management of peripheral artery disease has undergone major changes because percutaneous revascularization allows an alternative to open surgical repair. This is due at least in part to continued improvements and the invention of new techniques.2–7 Among these is the evolution of rotablation, atherectomy procedures, and laser-assisted angioplasty.4–8 Percutaneous transluminal angioplasty (PTA) is normally recommended as the primary treatment for short-segment femoropopliteal stenoses and occlusions.1–3,9 In contrast, lengthy chronic occlusions are still mainly treated surgically, especially those of the superficial femoral artery.1 Primary and secondary success rates of PTA still have various limitations. Vessel occlusion, long lesions, and the presence of vessel calcification decrease the technical success rates and long-term patency after recanalization with balloon angioplasty. Laser-assisted angioplasty was first evaluated in the late 1980s to overcome these limitations.10–15 The pulsed excimer laser has been extensively evaluated for its ability to debulk atherosclerotic material in vitro and in vivo, demonstrating that the photoablative effect of laser light can recanalize even lesions not amenable to conventional PTA.16–18 First experiences of the use of different laser systems raised high expectations for laser-assisted angioplasty, leading to extensive use of these new devices because the technical success rates, compared with PTA, were equal. The following years were filled with restraints toward laser angioplasty because there was no significant decrease in long-term restenosis rates.6,19,20 Percutaneous excimer laser–assisted revascularization has been shown to be an effective treatment for patients with claudication or chronic critical limb ischemia presenting in Rutherford stage 2 to 4. Patients with persistent symptoms for more than 6 months, a walking distance between 100 and 300 meters, and markedly reduced quality of life may also benefit from this technique. Single and multiple subtotal stenoses and occlusions in the iliac (Figs. e13-1 to e13-3), femoral (Figs. e13-4 and e13-5), and popliteal arteries can be treated with the laser when there is a suitable connecting vessel segment and sufficient runoff flow. Past experience shows that even long occlusions of more than 20 cm can be recanalized with technical success (see Figs. e13-4 and e13-5).8 The indication for excimer laser–assisted revascularization of a lesion should be based on either intraarterial digital subtraction angiography (IA-DSA) or contrast-enhanced magnetic resonance angiography (CE-MRA). After the first experiences with laser-assisted angioplasty in the early 1980s, only one laser system is employed today: the excimer laser. Two laser systems initially used or investigated were the Nd:YAG and CO2, both found to be either dangerous or ineffective for laser-assisted angioplasty. The Nd:YAG laser system showed a remarkable ablation rate of atherosclerotic material but led to heating of the artery wall, with a high risk of perforation and vessel destruction. In contrast, both the excimer and the CO2 lasers are “cold” laser systems that do not lead to heating at the treatment site, so the danger of vessel perforation due to lasing is negligible.21–27 Equipment required for laser-assisted angioplasty includes: • Excimer laser system (e.g., CVX 300 Laser System [Spectranetics Inc., Colorado Springs, Colo.]). • Laser catheters in appropriate sizes based on target vessel diameter. Currently, laser catheters are available as over-the-wire systems as well as rapid-exchange catheters. Sizes available range from 0.9 to 2.5 mm outer diameter of the catheter tip. Additionally, materials that are routinely used for peripheral interventions (e.g., introducer sheaths, catheters, PTA catheters, guidewires) are employed. Major target vessels for excimer laser–assisted angioplasty are the iliac and infrainguinal arteries, as well as the arteries below the knee (Fig. e13-6), among other vascular territories. For iliac artery occlusions, access depends on lesion length and location. In general, an occlusion in the external iliac artery should be treated in crossover approach (see Fig. e13-1). The occlusion of the common iliac artery (see Figs. e13-2 and e13-3) or occlusion of both common and external iliac arteries requires a bilateral access. First, these lesions are crossed in antegrade fashion with a guidewire, and then, after snaring the guidewire in the ipsilateral groin, the recanalization procedure is performed in a retrograde approach. Contralateral access with subsequent crossover recanalization of the occlusion can be considered the standard approach for recanalization of long superficial femoral artery occlusions (see Figs. e13-4 and e13-5).
Endovascular Laser Therapy
Indications
Equipment
Technique
Anatomy and Approaches
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Endovascular Laser Therapy